- [PART 1 of 2] Billy is a 16 year old male that jokingly takes his girlfriend’s pregnancy which subsequently turns positive. He thought this was rather unusual, so he decides to get checked out by his primary care physician. He is also experiencing gynecomastia. If the physician finds a testicular tumor, which of the following is most likely?
- Seminoma
- Yolk sac tumor
- Choriocarcinoma
- Teratoma
- Leydig cell tumor
- [PART 2 of 2] Billy is a 16 year old male that jokingly takes his girlfriend’s pregnancy which subsequently turns positive. He thought this was rather unusual, so he decides to get checked out by his primary care physician. He is also experiencing gynecomastia. If the physician finds a testicular tumor, which of the following would most likely be found on histology?
- Distorted Syncytiotrophoblasts
- Psammoma bodies
- Schiller-Duval Bodies
- Call-Exner bodies
- Necrosis
- A 4 year old male presents with a non-tender testicular mass. Labs show an increase in α-fetal protein. Which of the following would most likely bee seen on biopsy?
- Psammoma bodies
- Call Exner Bodies
- Reinke crystals
- Schiller-Duval Bodies
- Coffee bean nuclei
- A 67 year old female presents with abdominal pain for the last month. Last menstrual period was 10 years prior. Physical examination reveals a left adnexal mass and an ovarian biopsy is ordered. Histology shows proliferative, jagged lining with psammoma bodies. Which of the following would also be present in this patient and be most helpful in confirming the diagnosis?
- hCG
- α-fetoprotein
- Excess E2
- CA-125
- AFP
- A 67 year old female presents with ascites and pleural effusion. She also has a pelvic mass. She is diagnosed with Meigs syndrome. Which of the following types of tumors is most likely to be identified in this patient?
- Yolk sac carcinoma
- Choriocarcinoma
- Leydig Carcinoma
- Seminoma
- Fibroma
- Which of the following tumors is associated with Reinke crystals?
- Sertoli Tumor
- Leydig Tumor
- Choriocarcinoma
- Dysgerminoma
- Teratoma
- An ovarian tumor is biopsied and pathology identifies mucin secreting cells with signet ring morphology. You diagnose it as a krukenberg tumor. Which of the following is the most likely location of the primary tumor?
- Ovary
- Bone
- GI
- Lung
- Cervix
- A 32 year old female presents with bloody nipple discharge. A biopsy is performed. Which of the following is most likely to be found by the path lab?
- Well developed fibrovascular stalks and supported by myoepithelial cells
- A lack of myoepithelial cells
- Hypercellular stroma with leaf-like formation
- Cheesy necrotic material
- Mucin secretion with signet ring formation
- [PART 1 of 2] A 36 year old female patient presents to her OB-GYN with an erythematous, scaly red rash around her right nipple. Onset was approximately 2 weeks prior and patient was put on dicloxacillin by her PCP but doesn’t seem to help. Patient is 2 months postpartum and is currently breastfeeding. Breast is non-tender and is negative for edema. Patient vitals are within range and is afebrile. Which of the following is the most appropriate course of action?
- Perform an ultrasound-guided aspiration
- Order a mammogram
- Switch to Vancomycin
- Switch to TMP-SMX
- Advise patient to stop breastfeeding on affected breast
- [PART 2 of 2] What is the most likely diagnosis?
- Ductal cell carcinoma in situ
- Lobular cell carcinoma in situ
- Inflammatory breast carcinoma
- Acute mastitis
- Chronic mastitis
- A 26 year old male patient presents to the clinic with symptoms of inflammatory arthritis and conjunctivitis, and urethritis. Patient admits to having unprotected sex which prompts you to do further testing for STIs. Based on the symptomology, what is the most likely antibiotic combination you will use to combat the patients STI?
- Penicillin + Ceftriazone
- Cefriaxone + Azithromycin
- Azithromycin + Penicillin
- Penicillin alone
- Azithromycin alone
- You are trying to identify an unknown bacterium. It grows on chocolate agar and New York City Agar. It is positive for fermentation of glucose and maltose. Which of the following is most likely the identity of this bacterium?
- Chlamydia trachomatis
- Treponema pallidum
- Gardnerella vaginalis
- Neisseria gonorrhoeae
- Neisseria meningitidis
- Which of the following is NOT true regarding trichomonas vaginalis?
- It is usually asymptomatic, but can cause cervical petechiae when symptomatic
- It uses hydrogenosome which allows it to produce ATP without the presence of O2
- Decreased vaginal pH is a defining symptom
- NAAT is the preferred method of diagnosis
- IT will have a characteristic jerking/spinning motility on wet mount microscopy
- [PART 1 of 2] A 32 year old female presents with a pruritic maculopapular rash on the palms, soles and torso. She admits to having unprotected sex and you run a multitide of tests for various STIs. The tests come back positive for syphilis, as you expected. However, the patient is allergic to penicillin. What is the most appropriate course of treatment?
- Azithromycin
- Doxycycline
- Desensitize patient and utilize penicillin
- Ceftriaxone
- Pipercillin
- [PART 2 of 2] Which of the following tests would need to be positive to allow for a diagnosis of syphilis?
- RPR only
- TPPA and FTA-ABS
- VDRL and RPR
- RPR and TPPA
- FTA-ABS and MHA-TP
- Which of the following is characteristic for Haemophilus ducreyi infections?
- Railroad track appearance on gram stain
- Clue cells on wet mount microscopy
- Strawberry cervix
- Painless ulcers
- Donovan bodies
- Urinary canaliculi are often associated with which of the following STIs?
- Syphilis
- Mycoplasma
- Haemophilus ducreyi
- Klebsiella granulomatis
- Ureaplasma
- Which of the following is a viral pathogen that utilizes reverse transcriptase but is NOT a retrovirus?
- HIV-1
- HTLV-1
- HBV
- HCV
- HTLV-2
- Which of the following is associated with Adult T-cell Leukemia (ATL)?
- HTLV-1
- HTLV-2
- HIV-1
- HIV-2
- HPV
- Which of the following would distinguish bacillary angiomatosis from kaposi sarcoma?
- HHV-8 infection
- Patient has HIV
- Skin lesions
- Mixed infiltrate
- Angioproliferation
- A 24 year old, male patient presents with a headache, sore throat, fatigue and fever that began 2 weeks prior. The patient has a history of IV drug abuse and labs show drastically decreased CD4+ cells. Which of the following describes the virus responsible for this patient’s presentation?
- Single-stranded DNA
- Double-stranded DNA
- Single-stranded RNA
- Double-stranded RNA
- Drug compliance is extremely important in HIV+ patients due to the potential for drug resistance. Mutations in which of the following genes leads to HIV drug resistance?
- gag
- pol
- env
- CCR5
- CXC4
- What is the drug of choice in treating HIV+ patients with disseminated MAC?
- Azithromycin
- Clarithromycin
- Tobramycin
- Neomycin
- TMP-SMX
- One of your long-time patients, a 35 year-old male patient who is HIV+ presents to the clinic for a routine checkup. The patient has been overall well managed until recently when his CD4+ counts plummeted to less than 200. Additionally, he is recovering from a pneumocystis pneumonia for which the hospitalist prescribed TMP-SMX. While he has been able to fight the infection caused by PJP, you have concerns about the antibiotics prescribed resulting in which of the following problems?
- Acute kidney injury
- Liver failure
- Myocardial infarction
- Mitochondrial Toxicity
- Osteoporosis
- Which of the following tests need to be performed if a provider plans to prescribe Maraviroc to a HIV+ patient?
- HLA-B*5701 Test
- Tropism Test
- Heterophile Antibody Monotest
- CBC
- [PART 1 of 2] Which of the following drugs is used during pregnancy to decrease the risk of fetal transmission in an HIV+ mother?
- Abacavir
- Tenofovir
- Efavirenz
- Zidovudine
- Nevirapine
- [PART 2 of 2] Which of the following is a side effect from taking this medication?
- Mitochondrial Toxicity
- Nephrotoxicity
- Bone Marrow Suppression
- Hyperpigmentation
- Rash
- Which of the following combinations of drugs would be most appropriate to treat an HIV+ patient?
- Tenofovir, Didanosine, and Efavirenz
- Stavudine, Didanosine, and Darunavir
- Abacavir, Zidovudine, and Atazanavir
- Abacavir, Zidovudine, and Stavudine
- Stavudine, Zidovudine, and Ritonavir
- A 25 year old male patient presents to the clinic for a wellness exam. He is HIV+, but has been well controlled until recently. His viral load has been steadily increasing for the last 2 months and you are beginning to worry that this isn’t just a blip. The patient states that he has been compliant with his medications. He is also complaining of acid reflux for which he has been controlling with over-the-counter Prilosec (Omeprazole). Which of the following HAART medications is most likely being affected resulting in the increase in viral load?
- Atazanavir
- Etravirdine
- Didanosine
- Enfuvirtide
- Lopinavir
- A 32 year old female patient presents to the ER with symptoms of severe hypoxemia. The patient has a history of IV drug abuse. Labs show elevated LDH and CXR reveals diffuse, bilateral symmetrical ground glass interstitial infiltrates emanating from the hila in a butterfly pattern. Which of the following is the most appropriate immediate course of treatment?
- High dose TMP-SMX
- High dose fluconazole
- Begin HAART
- A & B
- B & C
- You are on rotations in the ICU when you come across a 45 year old male patient being treated for pneumocystis pneumonia. The attending has chosen to treat the patient with IV Pentamidine due to a sensitivity to TMP-SMX (the usual drug of choice). Your are monitoring the patient during the infusion when he becomes unresponsive. After notifying your attending, which of the following would be the most appropriate next step?
- Stop the infusion
- Check BGL
- Stop any HAART therapy
- Administer Insulin
- Perform vagal maneuver
- You are on rotations in the ICU when you come across a 42 year old male patient being treated for a disseminated Cryptococcus infection. The patient was recently diagnosed with HIV and initially presented with a headache and stiff neck. He has not yet been started on HAART. The patient was put on IV Amphotericin B + oral 5-Flucytosine to combat the infection. Currently, the patient’s opening pressure is 30 mm H2. The patient is experiencing mild confusion, blurred vision, and papilledema. Which of the following would be an additional treatment you could recommend in order to assist with the patient’s symptoms?
- Start HAART
- Change to high dose Fluconazole
- Daily lumbar punctures
- Drill burr holes
- Administer high dose steroids
- A 38 year old female patient who is HIV+ presents to the Emergency Department with headache, confusion, fever, and motor weakness. CD4+ counts are <200 and CT shows ring-enhancing lesions in the frontal and parietal lobes. The nurse notes that the patient lives alone and keeps asking for someone to check on her three cats while she is hospitalized. Which of the following is most likely responsible for her symptoms?
- Primary CNS lymphoma
- Cryptococcus neoformans
- Coccidioidomyces immitis
- Toxoplasma gondii
- Pneumocystis jirovecii
- [PART 1 of 2] Growth hormone insensitivity in a group of extremely rare genetic disorders in which the body in unable to use the GH that it produces. Laron syndrome, for example, is an autosomal recessive disorder characterized by insensitivity to GH, usually caused by a mutant GH receptor. Therefore, there is a failure of IGF-1 secretion in response to GH. Which of the following drugs would be most appropriate to treat this disorder?
- Somatotropin
- Mecasermin
- Octreotide
- Cosyntropin
- Pegvisomant
- [PART 2 of 2] Which of the following is a likely side effect from this drug?
- Hyperglycemia
- Hypoglycemia
- Thrombosis
- Acute renal failure
- Hot flashes
- Which of the following drugs is used to treat ITP (Immune thrombocytopenic purpura)?
- Somatotropin
- Mecasermin
- Octreotide
- Cosyntropin
- Pegvisomant
- Which of the following drugs can be used in the treatment of hyperprolactinemia?
- Mecasermin
- Pegvismant
- Cabergoline
- Leuprolide
- Nafarelin
- GnRH agonists are sometimes utilized in the treatment of infertility, but are much more often used in the suppression of gonadotropin release. Which of the following is a GnRH agonist?
- Ganirelix
- Cabergoline
- Pegvisomant
- Leuprolide
- Conivaptan
- Which of the following is utilized in the treatment of hypervolemic hyponatremia?
- Conivaptan
- Desmopressin
- Pitocin
- Ganirelix
- Pegvisomant
- Prostate cancer can be treated with which of the following drugs?
- Fluoxymesterone
- Testosterona enanthate
- Tamoxifen
- Flutamide
- Methyltestosterone
- Which of the following are secreted from the posterior pituitary?
- Oxytocin
- ADH
- PRL
- A & B
- A & C
- Adrenalectomy is an operation that removes one or both of the adrenal glands. In some cases, this is a necessary procedure to treat Cushing’s Disease. When this procedure has been performed, it can cause something called Nelson Syndrome. Which of the following would be a side effect of this condition?
- Bitemporal hemianopsia
- Hyperprolactinemia
- Infertility
- Acromegaly
- Hyperthyroidism
- What is the most common type of pituitary adenoma?
- Somatotroph adenoma
- Corticotroph adenoma
- Lactotroph adenoma
- Gonadotroph adenoma
- Thyrotroph adenoma
- A 42 year old male patient presents with with weight gain, high blood pressure, hyperglycemia, and fatigue. The patient is also experiencing centripetal obesity and a buffalo hump. Labs show and elevation in cortisol. You perform a dexamethasone suppression test, which doesn’t seem to affect the cortisol levels. Which of the following is most likely responsible for the patients symptoms?
- Cushing’s Disease
- Pituitary Adenoma
- Pheochromocytoma
- Addison’s Disease
- Hashimoto’s Thyroiditis
- A pathologist sends you back the analysis of a hypothalamic suprasellar tumor, but neglects to say the diagnosis. The tumor is described as a “discrete, encapsulated mass” which is “not densely adherent to adjacent brain.” A mutation in which of the following is most likely associated with this tumor?
- BRAF V600E
- CDKN1B
- Cyclin D1
- HRAS
- CTNNB1
- A 17 year old female presents to you clinic and states that she is scared she might be pregnant after having intercourse with her boyfriend the previous night. She is asking for an emergency contraceptive. Which medication would be most appropriate to prescribe?
- Progesterone
- Norethindrone
- Norgestimate
- Mifepristone
- Exemestane
- A 30 year old female presents to the clinic complaining of LBP following attempting a heavy deadlift at the gym. After imaging and a physical, you decide that her muscle is only strained. You prescribe NSAIDs. If the patient has a history of stomach ulcers, which of the following drugs would be beneficial to also prescribe?
- Mifepristone
- Dinoprostone
- Misoprostol
- Latanoprost
- Ulipristal
- The use of St John’s Wort can cause subtherapeutic levels of all except which of the following drugs?
- Theophylline
- Sertraline
- Digoxin
- Cyclosporin
- Warfarin
- Which of the following is associated with vitamin A deficiency?
- Skin xerosis
- Alopecia
- Bone loss
- Nyctalopia
- Neonatal Hemorrhage
- A 27 year old presents to the clinic for a woman’s wellness visit. She explains that her and her husband are wanting to conceive. Her husband was born with spina bifida and she is concerned about neural tube defects for their future children. She asks you how long and at what dose she should be taking folate before trying to conceive. What should you tell her?
- 2 months, 4mg/day
- 2 months, 1mg/day
- 1 month, 4 mg/day
- 1 month, 1 mg/day
- 6 months, 1 mg/day
- A 46 year old male patient presents to the clinic for a wellness exam. She has a BGL of 220 and you diagnose her with Type II diabetes. You counsel her on the appropriate diet and necessity of exercise in addition to prescribing Metformin. Which of the following vitamins are you going to also encourage the patient to take?
- Vitamin B6
- Vitamin B3
- Vitamin B1
- Vitamin B12
- Vitamin C
- All of the following should be supplemented when prescribing proton pump inhibitors EXCEPT which?
- Fe
- Mg2+
- Ca2+
- B12
- K+
- Which of the following drugs should be utilized for mercury poisoning?
- Succimer
- Penicillamine
- Deferasirox
- Dimercaprol
- EDTA
- A 22 year old female presents to the clinic with cystic acne that has yet to completely resolve with conventional antibiotics. You decide to add Isotretinoin to her treatment regimen. Which of the following should be your next course of action before allowing her to take this medication?
- Pregnancy test
- Ultrasound
- Add an iron supplement
- Test TSH
- Ask about herbal supplements
- A 32 year old pregnant female presents 41 weeks term. You decide to induce her due to the risks associated with post-term labor utilizing IV oxytocin. High doses of oxytocin can be associated with which of the following?
- Hyponatremia
- Hyperpigmentation
- Weight Gain
- Decreased bone density
- Thrombosis
- A 32 year old male presents with a diffuse goiter of which the patient noticed a week prior. Patient is complaining of fatigue and weight gain. Dexamethasone suppression and cosyntropin tests were normal. Labs show elevated TSH and low T3/T4. Which of the following is the most likely diagnosis of this patient?
- TSH secreting adenoma
- Graves Disease
- Hashimoto’s Thyroiditis
- Non-functional pituitary adenoma
- Iodine deficiency
- Thyrotoxicosis should be managed with all EXCEPT which of the following?
- Beta Blockers
- NSAIDs
- Cholestyramine
- Radioiodine
- Levothyroxine
- A 23 year old female patient with thyrotoxicosis and a history of asthma presents to the clinic. The patient is experiencing weight loss, insensitivity to heat, and tachycardia. You decide to treat with Methimazole (the patient denies pregnancy), NSAIDs, and Cholestyramine. Which of the following drugs would be most appropriate in treating the patients high heart rate?
- Diltiazem
- PTU
- Levothyroxine
- Propranolol
- Amiodarone
- Which of the following drugs is most appropriate to treat a pregnant patient (first trimester) with hyperthyroidism?
- Methimazole
- Propylthiouracil
- Carbimazole
- Levothyroxine
- Dessicated thyroid
- A patient presents with symptoms of cortisol excess including striae, moon facies, and a dorsal fat pad. The patient denies any use of exogenous corticosteroids. Dexamethasone suppression test reveals that cortisol is decreased in response to high dose dexamethasone. Which of the following should be performed to distinguish between a pituitary and ectopic ACTH suppression?
- Inferior petrosal sinus sampling
- Cosyntropin response test
- TSH response test
- Ultrasound
- Fine needle aspiration of pituitary
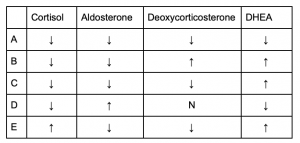
- [PART 1 of 3] Which of the following correctly describes the lab values of a patient with a 21 hydroxylase deficiency?

- A
- B
- C
- D
- E
- [PART 2 of 3] Which of the following correctly describes the lab values of a patient with a 17 hydroxylase deficiency?
- A
- B
- C
- D
- E
- [PART 3 of 3] Which of the following correctly describes the lab values of a patient with a 11β hydroxylase deficiency?
- A
- B
- C
- D
- E
- A patient presents with moon facies, buffalo hump, diarrhea, and hypokalemia indicative of dehydration. Labs show elevated calcitonin. Calcium levels are 8.8 mg/dL (Normal 8.6-10.3 mg/dL). Patients vitals are all within normal range. Physical examination reveals a solitary thyroid nodule and FNA is ordered. Which of the following is the most likely diagnosis?
- Papillary Thyroid carcinoma
- Medullary Thyroid carcinoma
- Pheochromocytoma
- Anaplastic Thyroid carcinoma
- MEN Type 1
- Which of the following is a likely presentation with someone with MEN Type I?
- Hypertension
- Gastric ulcers
- Elevated calcitonin
- Marfan like habitus
- Hypocalcemia
- Which of the following is a likely presentation with someone with MEN Type 2A?
- Hypoglycemia
- Gastric ulcers
- Neuromas
- Hypertension
- Acromegaly
- Which of the following is a likely presentation with someone with MEN Type 2B?
- Hypoglycemia
- Gastric ulcers
- Hyperextensibility of joints
- Acromegaly
- Hypercalcemia
- A 42 year old female patient presents with hypercalcemia, the cause of which is determined to be a parathyroid adenoma producing excess PTH. Upon further examination, the patient has multiple other endocrine neoplasms including a lactotroph adenoma. Genetic testing reveals an inactivating mutation in MEN1 tumor suppressing gene. Which of the following is this patient also likely to presenting with?
- Peptic ulcers
- Pheochromocytoma
- Medullary Thyroid carcinoma
- Hyperextensibility of joints
- Neuroma
- Which of the following would be a likely presentation for a patient with a glucagonoma?
- Hypoglycemia
- Peptic ulcers
- Hypertension
- Hypokalemia
- Migratory necrolytic erythema
- 25 year old female patient presents with skin lesions and diarrhea. Patient was put on Nacin (B3) supplements by her primary care physician 2 months prior, but symptoms have yet to subside. Labs reveal elevated 5-HT. Which of the following is a likely diagnosis?
- Carcinoid
- Insulinoma
- Glucagonoma
- Pheochromocytoma
- Pellagra
- Which of the following is highly associated with Type II Diabetes?
- Amyloid deposition
- Autoimmune destruction of β-cells
- DKA
- HLA-DR-3
- Weight loss
- Which is the first line of treatment for Type II Diabetes Mellitus in conjunction with diet and exercise?
- Acarbose
- Glyburide
- Metformin
- NPH
- Sitagliptin
- [PART 1 of 2] A 52 year old male patient presents to the clinic requesting a change in medication. He was previously diagnosed with Type II Diabetes and was prescribed Metformin. He is complaining that this medication is causing nausea and diarrhea which inhibits his day to day function. The patient has a BMI of 35%. The patient also has a history of CHF. Which of the following drugs would be most appropriate to prescribe this patient?
- Exenatide
- Glyburide
- Sitagliptin
- Pioglitazone
- Acarbose
- [PART 2 of 2] What is the mechanism of action for the drug chosen in part 1 of this question?
- Increases insulin sensitivity
- Incretin analog
- Inhibits PPAR𝝲
- Inhibits ATP-dependent K+ channels
- Inhibits DPP-4
- A 34 year old woman reports to your office for a well woman exam. The patient history is significant for menarchy at age 12, coitarchy at age 14, and a history of multiple sexual partners. She is complaining that lately she sometimes has postcoital spotting. Exam shows no cervical discharge, and Pap smear reveals the presents of koilocytes. Which of the following agents is likely causing the patient’s symptoms?
- Chlamydia trachomatis
- Treponema pallidum
- Trichomonas vaginalis
- HPV
- HSV
- A 58 year old woman comes to your clinic complaining of breast tenderness. She is concerned that she may have breast cancer, as her mother and grandmother did. History reveals newly onset vaginal bleeding, although her last menstruation was 3 years ago. On physical exam, you are able to palpate a unilateral adnexal mass. Endometrial biopsy shows signs of hyperplasia. The likely cause of these findings would be which of the following?
- Adverse drug effect
- Granulosa cell tumor
- Endometrial carcinoma
- Leiomyosarcoma
- Fibroma
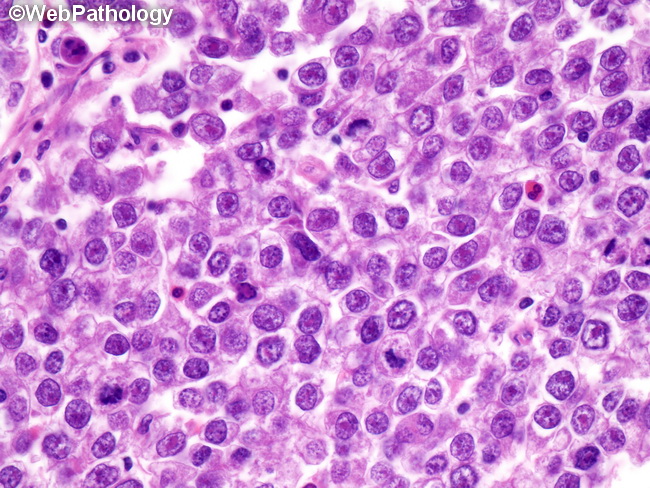
- A 17 year old female patient complaining of general abdominal discomfort and difficulty tolerating heat is revealed to have a firm adnexal mass on physical exam and labs return with elevated hCG and LH.
A surgical consult results in the ultimate removal of an ovarian mass. Pathology shows the exhibit below. What was the final diagnosis for this patient?- Dysgerminoma
- Yolk Sac Tumor
- Embryonal Tumor
- Choriocarcinoma
- Endodermal sinus tumor
- A 23 year old female presents to your office complaining of irregular menstruation hoping to get help regulating her periods. Physical exam reveals a well developed female of seemingly good health with a BMI of 21, with coarse hair above the upper lip and on the chest. Vital signs show a HR of 72 and BP of 145/86 with a temperature of 98F. Which of the following would be the most likely adrenal enzyme deficiency in this patient, were she to have one?
- 17α-Hydroxylase
- 21-Hydroxylase
- 11β-Hydroxylase
- 3β-HSD
- Aromatase
- Which of the following would directly cause an increase in secretion of PTH?
- Increased serum calcium
- Decreased serum phosphate
- Low serum magnesium
- Increased serum potassium
- Decreased serum sodium
- Elevated appetite, blood pressure, and gluconeogenesis with marked eosinopenia could indicate a functional lesion in which area?
- Adrenal zona glomerulosa
- Adrenal zona fasiciculata
- Adrenal zona reticularis
- Adrenal medulla
- Posterior pituitary gland