
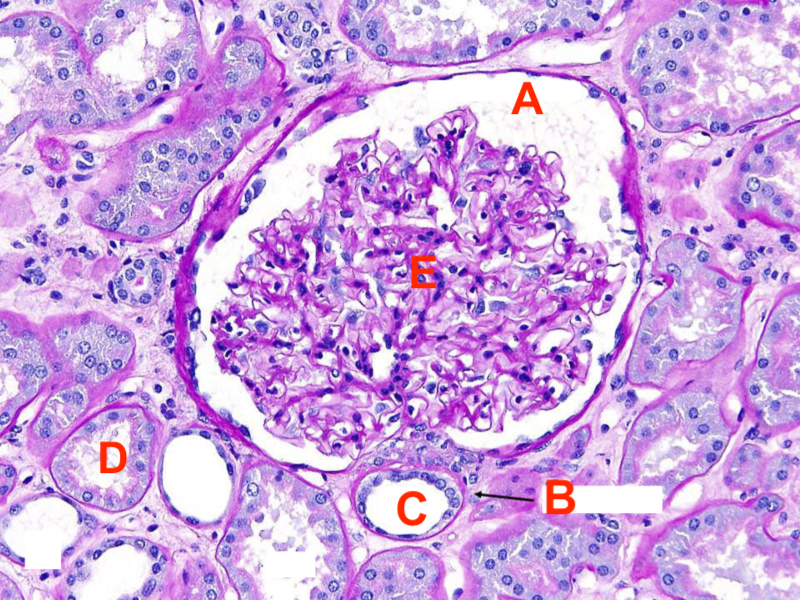
- The picture below depicts a microscopic view of the renal cortex. Approximately 75% of water and sodium reabsorption occurs at which structure?

- A
- B
- C
- D
- E
Answer D. Most sodium and water reabsorption occurs at the PCT. The PCT is darker staining compared to the DCT and has a more cloudy appearance.
A: Bowman’s Capsule.
B: Vasa Recta.
C: Distal Convoluted Tubule.
E: Glomerulus.
- You are on rotations with a pathologist and are looking at a micro-pictograph of a kidney. The pathologist points to a structure with simple squamous epithelium and asks you what structure it could be. What would be the best answer?
- Proximal convoluted tubule
- Distal convoluted tubule
- Collecting duct
- Thick loop of Henle
- Thin loop of Henle
Answer E. The thin portion of the loop of Henle and parietal layer of the Bowman’s capsule have simple squamous epithelium.
- Which of the following is true regarding urothelium?
- Umbrella cells will appear more bulbous when the bladder is full
- The urothelium will consist of 5-7 layers when the bladder is full
-
Transitional epithelium can be found in the lungs, uterus, and bladder and is vital for the expansive quality of these organs
-
Uroplakins are vital in forming an osmotic barrier that protect underlying cells and tissues from urine
-
The urothelium is part of the submucosal layer of the bladder
Answer D.
Lecture #58: Renal System Development
Which of the following embryological structures will become the functional and fully matured kidneys?
-
Pronephros
-
Mesonephros
-
Metanephros
-
Nephrogenic Cord
-
Urogenital Ridge
Answer C.
You are practicing ultrasound on a classmate but are having difficulty locating their right kidney. A physician comes over to assist you, and after even they are unable to locate it, they tell you that this classmate might have unilateral kidney agenesis. Which of the following embryological structures has failed to form in your peer?
-
Cloaca
-
Allantois
-
Metanephrogenic blastema
-
Metanephric diverticulum (Ureteric Bud)
-
Urachus
Answer D.
A patient presents to the clinic complaining of dysuria and increased frequency in urination. She believes she has a UTI and explains that this will be the 3rd one this year. You want to do further testing to investigate this and decide to order a CT scan. Ultrasonography reveals that the kidneys have been arrested at the level of the inferior mesenteric artery. Which of the following conditions is most likely leading to her recurrent UTIs?
-
Horseshoe Kidney
-
Unilateral renal agenesis
-
Potters Syndrome
-
Pelvic Kidney
-
Duplex kidney
Answer D.
You are on OB-GYN rotations in 3rd year when you encounter a newborn male patient displaying exstrophy of the bladder. The patient has protrusion of the mucosal surface of the posterior bladder wall, leaving the trigone of the bladder exposed. The trigone of the bladder develops from which of the following embryological structures?
-
Urogenital sinus
-
Allantois
-
Mesonephric ducts
-
Urachus
-
Cloaca
Answer C. Although the majority of the bladder arises from the urogenital sinus, the trigone comes specifically from the mesonephric ducts.
You are on OB-GYN rotations in 3rd year when you encounter a newborn male patient that has urine leaking from his umbilicus. Which of the following conditions is most likely characteristic of this issue?
-
Urachal fistula
-
Urachal cyst
-
Exstrophy of the bladder
-
Epispadias
-
Pelvic Kidney
Answer A.
B59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
Congenital nephrotic syndrome is a kidney condition that begins in infancy and typically leads to irreversible kidney failure by early childhood. Children with this disease are deficiency in Nephrin, a protein that is vital for providing transmembrane support to the slit diaphragm. If you suspected a child to have this disease, which of the following symptoms would assist in your diagnosis?
-
Hematuria
-
Proteinuria
-
Glycosuria
-
Hypercalciuria
-
Pyuria
Answer B. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
Diabetic nephropathy causes characteristic changes to the structure of the glomerulus by disrupting the podocyte cytoskeleton, and can even lead to the complete loss of podocytes. Which of the following is a potential outcome of individuals with this disease?
-
GFR will be increased
-
GFR will be unchanged
-
Creatinine levels will decrease
-
Creatinine levels will remain unchanged
-
Plasma oncotic pressure will increase
Answer A. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
Lisinopril is an ACE inhibitor often prescribed to patients with hypertension and works to cause vasodilation of the efferent arterioles. Based on this information, which of the following is a likely outcome from Lisinopril?
-
Increased Glomerular Filtration Rate
-
Unchanged Glomerular Filtration Rate
-
Increased Net Filtration Pressure
-
Decreased Net Filtration Pressure
-
Increased Filtration Fraction
Answer D. Answer A. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
Kwashiorkor is a nutritional disorder caused by a protein deficiency and is most often seen in regions experiencing famine. People who have kwashiorkor typically have an extremely emaciated appearance with localized swelling in their ankles, feet and stomach. Which of the following is most likely diminished in a patient with this deficiency?
-
Glomerular Capillary Hydrostatic Pressure (PG)
-
Plasma Oncotic Pressure (πG)
-
Bowman’s Capsule Hydrostatic Pressure (PB)
-
Bowman’s Capsule Oncotic Pressure (πB)
-
Filtration Coefficient (Kf)
Answer B.Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
Inulin is the most accurate measurement of glomerular filtration rate (GFR). However, the steps involved in its measurement are often quite involved. Therefore, Creatinine is more often utilized to measure GFR. Which of the following is NOT true regarding Creatinine?
-
Creatinine clearance declines with age
-
A long term change in GFR is needed to affect plasma creatinine levels
-
A patient can be exhibiting nephropathy without an affect on plasma creatinine levels
-
Creatinine is partially secreted
-
Creatinine is often under-assessed in the plasma
Answer E. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
You diagnose a 54 year old woman with syndrome of inappropriate ADH (SIADH). Which laboratory results would support your diagnosis?
-
Urine specific gravity of 1.004
-
Creatinine level of 2.0
-
Elevated urine Na+ level
-
Serum Na+ level of 140 mEq/L (normal 135-145 mEq/L)
-
Decreased urine osmolality
Answer C. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
A defect in the gene for nephrin, NPHS1, is associated with congenital nephrotic syndrome of the Finnish type. What would you expect to see in a patient with this congenital defect?
-
Proteinuria
-
Hyponatremia
-
Hematuria
-
Hypokalemia
-
Hyperalbuminemia
Answer A. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
The glomerular filtration rate of glucose is __________ the excretion rate of glucose.
-
Less than
-
Equal to
-
Greater than
-
2 times
-
½
Answer B. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
A 63 year old man presents to you with muscle weakness and recurrent headaches. Following a full work-up and history, you determine that he is hyponatremic, which is causing his symptoms. He has a history of diabetes, diabetic nephropathy, and chronic renal disease. Blood pressure: 128/78, RR: 18, HR: 82. He is currently undergoing dialysis 4 times per week. What could be contributing to his hyponatremia?
-
Decreased secretion of sodium
-
Increased net filtration pressure
-
Decreased glomerular filtration of water caused by diabetic nephropathy
-
Increased Na+ reabsorption in the distal convoluted tubule
-
Dehydration
Answer C. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
Given the below values, which of the following most closely represents the GFR?
Filtration Rate Coefficient = 12.5 mL/min
Glomerular Capillary Hydrostatic Pressure = 75 mm Hg
Plasma Oncotic (Colloid) Pressure = 20 mm Hg
Bowman’s Capsule Hydrostatic Pressure = 15 mm Hg
-
250 mL/min
-
500 mL/min
-
560 mL/min
-
600 mL/min
-
750 mL/min
Answer B. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
A patient presents to your clinic complaining of water retention. After a full work-up, you prescribe the patient Methazolamide, a commonly prescribed diuretic which inhibits the activity of carbonic anhydrase. By which mechanism is this medication able to improve the patient’s condition?
-
It decreases reabsorption of bicarbonate, which decreases the activity of the apical Na+/H+ exchanger, causing retention of Na+ in the filtrate.
-
It increases production of CO2, which is passively reabsorbed, and increases retention of Na+ in the filtrate.
-
It decreases production of H+ in the proximal convoluted tubule, which leads to inactivation of the Na+/K+ pump, leading to retention of Na+ in the filtrate.
-
It inhibits the formation of carbonic acid, which decreases the activity of the apical Na+/K+ pump, leading to retention of Na+ in the filtrate.
-
It inhibits the Na+/H+ pump, leading to decreased reformation of bicarbonate, resulting in decreased Na+ in the filtrate.
Answer A. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
Which of the following is true regarding pressure gradients along a glomerular capillary in a normal, healthy individual?
-
Afferent PGC > Efferent PGC
-
Afferent PGC < Efferent PGC
-
Afferent PGC < Efferent PGC
-
Afferent COP < Efferent COP
-
Afferent COP > Efferent COP
Answer E. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
The filtrate becomes more dilute as it progresses through the thick ascending loop of Henle. What characteristics of the ascending limb are responsible for this?
-
The ascending loop of Henle is permeable to water and ions.
-
The ascending loop of Henle is impermeable to water and ions.
-
The ascending loop of Henle is permeable to ions but impermeable to water
-
The ascending loop of Henle is impermeable to ions and urea.
-
The ascending loop of Henle is permeable to water and urea.
Answer C. Lecture #59-61: Glomerular Filtration & Renal Blood Flow I, II, & III
B62: MHC Restriction
Which of the following is TRUE in regards to positive selection of T-cells?
-
Positive selection of T-cells takes place in the bone marrow
-
Positive selection promotes proficient central tolerance
-
If the TCR interacts with MHC I on cTEC, then CD8+ will be downregulated
-
Thymocytes expressing a transgenic allele restricted to a particular MHC allele will not mature or emigrate from the thymus
-
Positive selection occurs before V(D)J recombination
Answer D.
A donor CD4+ T-cell recognizes allogeneic MHC after its been phagocytized and presented in the context of self MHC II. This describes alloreactive activation of a T-cell through which of the following pathways?
-
Indirect
-
Direct
-
Semi-indirect
-
Semi-direct
-
Conservative
Answer A. Lecture #62: MHC Restriction
A 23 year old female patient with B- blood type presents to the Emergency Department in need of a blood transfusion following a MVA. Unfortunately, her blood type is incorrectly recorded and she is given A- blood instead. Which of the following rejection types is most likely to occur?
-
Chronic
-
Acute
-
Hyperacute
-
Semi-acute
-
Semi-chronic
Answer C.
HLA-typing is most important in which of the following transplants?
-
Liver
-
Heart
-
Kidney
-
Hematopoietic Stem Cells (HSC)
-
Lung
Answer D.
Total body irradiation is used to eliminate the Leukemia and, in the case of allogeneic transplant, to suppress the patient’s immune system in preparation for the transplanted stem cells. In order to decrease the incidence of infections following HSCT, which of the following could be given?
-
Corticosteroids
-
Cyclosporine
-
Rapamycin
-
IL-2 Blockade
-
G-CSF
Answer E. G-CSF will stimulate myeloid cell regeneration while all the other answers are immunosuppressants. Lecture #62: MHC Restriction
B63-64: Tubular Reabsorption & Secretion I/II
Which of the following is an example of symport secondary active transport?
-
SGLT
-
H+ ATPase
-
Na+ K+ ATPase
-
ROMK
-
NHE3
Answer A.
Which part of the Loop of Henle is only permeable to water?
-
Proximal convoluted tubule
-
Distal convoluted tubule
-
Thick ascending limb
-
Descending limb
-
Thin ascending limb
Answer C. Lecture #63-64: Tubular Reabsorption & Secretion I/II
“Substrate X” is freely filtered at the glomerulus and, under normal circumstances, 100% is reabsorbed in the PCT via secondary active transport. Substrate X is not secreted, but can be found in the urine if the concentration is high enough. Given the following renal titration curve, which of the following is closest to the transport maximum of the secondary active transporter used to reabsorb Substrate X?
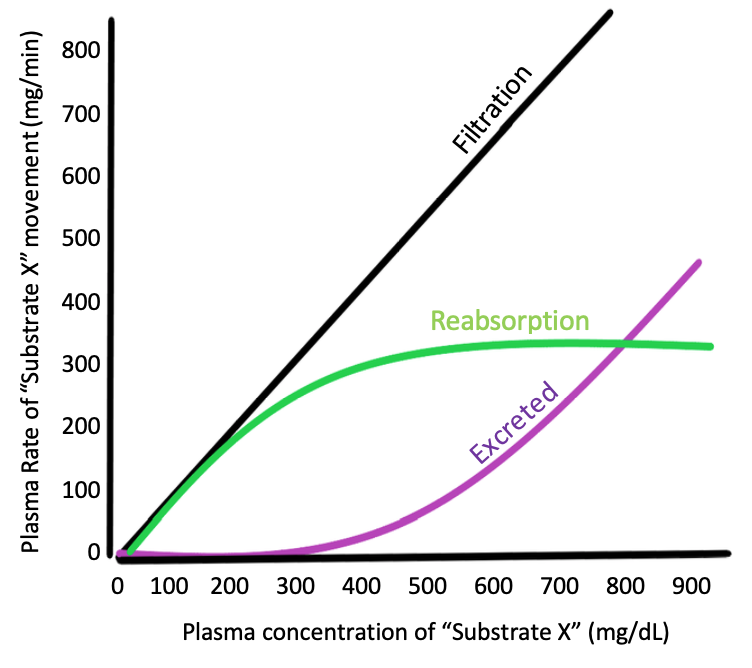
-
300 mg/min
-
800 mg/dL
-
400 mg/min
-
200 mg/dL
-
50 mg/min
Answer A.
“Substrate X” is freely filtered at the glomerulus and, under normal circumstances, 100% is reabsorbed in the PCT via secondary active transport. Substrate X is not secreted, but can be found in the urine if the concentration is high enough. Given the following renal titration curve, which of the following is closest to the threshold maximum of Substrate X?
-
300 mg/min
-
800 mg/dL
-
400 mg/min
-
use
-
50 mg/min
Answer D.
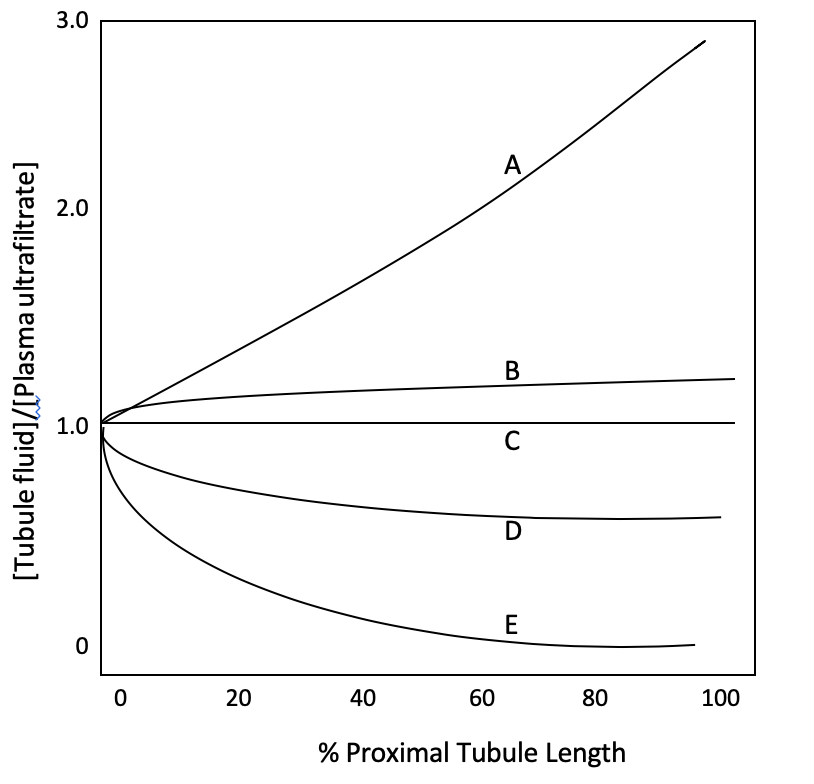
A substrate is freely filtered at the glomerulus, but nearly 100% of it is reabsorbed at the PCT. Which of the following best represents this substrate?
-
A
-
B
-
C
-
D
-
E
Answer E.
Which of the following substrates would be best to utilize in measuring GFR?
-
A
-
B
-
C
-
D
-
E
Answer A.
Which of the following is TRUE regarding PCT?
-
The majority of potassium secretion occurs here
-
At the end of the PCT, the filtrate is hyperosmotic
-
At the end of the PCT, the filtrate is hypoosmotic
-
Around 65% of Na+ reabsorption occurs here
-
SGLT is the most important transporter for Na+ reabsorption
Answer D.
Which of the following diuretics work by utilizing the osmotic gradient of water oppose to acting directly on a transporter?
-
Thiazides
-
Amiloride
-
Lasix
-
Dorzolamide
-
Mannitol
Answer E.
MK-7145, an Oral Small Molecule ROMK Inhibitor, has been used in trials studying the treatment of Hypertension and Renal Insufficiency. Which of the following could be a potential side effect of this molecule?
-
Hypercalcemia
-
Hypernatremia
-
Hypoglycemia
-
Hypomagnesemia
-
Alkalosis
Answer D.
Which of the following is TRUE regarding the molarity of filtrate at the beginning of the loop of henle as oppose to the end?
-
The beginning is hyperosmotic and the end is hyposmotic
-
The beginning and end are both isosmotic
-
The beginning is isosmotic and the end is hyposmotic
-
The beginning is isosmotic and the end is hyperosmotic
-
The beginning is hyposmotic and the end is hyperosmotic
Answer C.
Uncontrolled Diabetes mellitus is often associated with polyuria (excessive urination). Which of the following BEST explains the reasoning behind this?
-
High BGL causes osmotic flow to favor water movement into the PCT
-
High BGL causes osmotic flow to favor water movement into the blood
-
High BGL directly inhibits aquaporins the located in the PCT, disfavoring water reabsorption
-
High BGL directly inhibits aquaporins the located in the PCT, favoring water reabsorption
-
High BGL causes polydipsia which leads to increased fluid intake
Lactic acidosis is a common finding in critically ill patients during severe septic shock, and a powerful predictor of mortality. How would this interfere with a patient being treated with a negatively charged antibiotic like Penicillin?
-
Acidosis would allow PCN to take a neutral charge and encourage reabsorption of the drug
-
Acidosis would allow PCN to take a neutral charge and and encourage secretion of the drug
-
Acidosis would allow PCN to take a positive charge and and encourage secretion of the drug
-
Acidosis would allow PCN to take a positive charge and encourage reabsorption of the drug
-
Acidosis would allow PCN to take a negative charge and and encourage secretion of the drug
Answer A. Lecture #63-64: Tubular Reabsorption & Secretion I/II
Inulin and para-amino hippuric acid (PAH) are administered to your patient. The following measurements were made during the course of the infusion, and were noted to be constant
throughout the experiment: arterial plasma concentration of inulin = 0.18 mg/ml, arterial plasma concentration of PAH = 0.2 mg/ml; renal venous plasma concentration of PAH = 0.0015
mg/mL; urine flow 3 mL/min; urinary concentration of inulin = 9.0 mg/mL, urinary concentration of PAH = 50 mg/mL. Calculate the inulin clearance.
-
150 mL/min
-
180 mL/min
-
120 mL/min
-
225 mL/min
-
135 mL/min
Answer A.
Inulin and para-amino hippuric acid (PAH) are administered to your patient. The following measurements were made during the course of the infusion, and were noted to be constant
throughout the experiment: arterial plasma concentration of inulin = 0.18 mg/mL, arterial plasma concentration of PAH = 0.22 mg/mL; renal venous plasma concentration of PAH = 0.0015
mg/mL; urine flow 3 mL/min; urinary concentration of inulin = 9.0 mg/mL, urinary concentration of PAH = 50 mg/mL. Calculate the transport maximum (Tm) for PAH.
-
11 mg/min
-
117 mg/min
-
150 mg/min
-
139 mg/min
-
PAH is secreted. The transport maximum cannot be determined.
Answer B. Tm = UPAH x V – GFR x PPAH 50mg/mL x 3 mL/min – 150 mL/min x 0.22 mg/mL
Inulin and para-amino hippuric acid (PAH) are administered to your patient. The following measurements were made during the course of the infusion, and were noted to be constant
throughout the experiment: arterial plasma concentration of inulin = 0.18 mg/mL, arterial plasma concentration of PAH = 0.25 mg/mL; renal venous plasma concentration of PAH = 0.0015
mg/mL; urine flow 3 mL/min; urinary concentration of inulin = 9.0 mg/mL, urinary concentration of PAH = 50 mg/mL. Calculate the renal plasma flow (RPF) for PAH.
-
135 mL/min
-
150 mL/min
-
360 mL/min
-
420 mL/min
-
600 mL/min
Answer E. RPF = UPAH x V / (arterialPAH – venousPAH)
= 50mg/mL x 3 mL/min / (0.25 mg/mL – 0.0015 mg/mL)
______________ is a hormone that plays a role in the distal convoluted tubule. The release of this hormone causes Na+ reabsorption, which, in turn, causes water reabsorption.
-
ANP
-
Aldosterone
-
PAH
-
Testosterone
-
PTH
Answer B.
The primary purpose of the Loop of Henle is
-
Maintain an isotonic environment in the renal medulla
-
Concentrate the urine by allowing reabsorption of water and sodium chloride from the filtrate
-
Dilute the urine by secreting water and sodium chloride into the filtrate
-
Assist the Proximal Convoluted Tubule with hydrogen ion secretion to maintain normal blood pH
-
Dilute the urine by reabsorbing water and sodium chloride from the filtrate
Answer B.
B65: T Cells II, Cell Cooperation & Cytokines
You are doing clinical rotations in a family practice clinic when a patient presents with Nausea, weakness, loss of appetite, abdominal pain, diarrhea, and dizziness. Upon further testing, you come to find that the patient has an adult tapeworm living within their intestines. Which of the following cytokines would be secreted by NKs to signal the differentiation of naive T-cells?
-
IL-12
-
IL-4
-
TGF-β
-
IL-17
-
IL-23
Answer B.
Tuberculosis is an infection caused by Mycobacterium tuberculosis. Which of the following cytokines would be secreted by NKs to signal the differentiation of naive T-cells in this disease?
-
IL-12
-
IL-4
-
TGF-β
-
IL-17
-
IL-23
Answer A. Lecture #65: T Cells II, Cell Cooperation & Cytokines
A deficiency in which of the following cytokines could diminish peripheral tolerance and thus has the potential to cause autoimmune disease?
-
IL-17
-
IL-4
-
INF-λ
-
IL-1
-
TGF-beta
Answer E. TGT-beta is responsible for signaling Regulatory T-cells which are responsible for maintaining peripheral tolerance. Studies suggest that problems with TGF-beta have been linked with a number of autoimmune diseases.
Chronic mucocutaneous candidiasis (CMC) refers to a heterogeneous group of disorders characterized by recurrent or persistent superficial infections of the skin, mucous membranes, and nails with Candida organisms. CMC is a common manifestation of deficiency Th17 immunity. Which of the following diseases is LEAST likely to be associated with CMC?
-
APECED
-
AR-HIES
-
AD-HIES
-
Autoimmune polyendocrinopathy
-
X-SCID
Answer E. All others are associated with deficient Th17 immunity.
A patient has presented to the allergist complaining of multiple allergic reactions to seemingly unrelated foods. Testing reveals that the patient is allergic to a multitude of common allergens. If the physician suspects immune disease, which of the following would most likely be defective?
-
Th1 immunity
-
Th2 immunity
-
Th17 immunity
-
Treg immunity
-
Tfh immunity
Answer B. Lecture #65: T Cells II, Cell Cooperation & Cytokines
A 23 year old patient presents to the clinic with a sinus drip and epiphora (watery eyes). History reveals that the patient has seasonal allergies (aka hay fever). Which of the following cytokines is most likely directly responsible for this patient’s symptoms?
-
IL-4
-
IL-5
-
IL-13
-
IL-23
-
INF-λ
Answer C.
IPEX (immunodysregulation polyendocrinopathy enteropathy X-linked) syndrome is a rare disease linked to the dysfunction of the transcription factor FOXP3. Which of the following t-cell types are most likely going to be affected by IPEX?
-
Th1
-
Th2
-
Th17
-
Treg
-
Tfh
Answer D.
Which of the following T-helper subtypes is most ideal for eliminating tumors?
-
Th1
-
Th2
-
Th17
-
Tfh
-
Treg
Answer A.
Which of the following has the greatest potential to be utilized as a therapeutic agent in cancer?
-
IL-4
-
IL-5
-
IL-13
-
IL-23
-
INF-λ
Answer E. Lecture #65: T Cells II, Cell Cooperation & Cytokines
B66-67: B Lymphocytes I & II
A 6 month old male patient presents to your clinic with recurrent otitis (ear infection) and bronchitis (lung infection). You decide to run some tests (Bruton Tyrosine Kinase (BTK) Genotype and Protein Analysis, Full Gene Sequence and Flow Cytometry). You find that his B cell count is low and he has a mutation in the Btk gene. What is your diagnosis?
-
X-linked agammaglobulinemia
-
Coronary artery disease
-
Severe combined immunodeficiency
-
Chronic granulomatous disease
-
X-linked hyper IgM
Answer: A.
Which of the following cell types are responsible for presenting whole, unprocessed antigen to B-cells in the lymph node?
-
Subcapsular Macrophages
-
Follicular Dendritic Cells
-
Conventional Dendritic Cells
-
A & B
-
A, B & C
Answer D. Lecture #66-67: B Lymphocytes I & II
When antigen binds to a B cell receptor, which of the following is involved in the transduction of signal 2 by the B cell?
-
CD40L
-
CD80
-
CD53
-
CR2
-
CD79
Answer: B.
A HIV-positive mother becomes pregnant and wants to see if the child is at risk for infection. The father has been tested and has a mutation in the CCR5 gene that provides resistance to HIV infection. You perform genetic testing, and the child has inherited the mutation that can provide resistance to the infection. Which mechanism is responsible for the expression of this mutation?
-
Central tolerance
-
Peripheral tolerance
-
BCR cross-linking
-
Isotype exclusion
-
Allelic exclusion
Answer E.
You perform a renal biopsy on one of your cancer patients. Under microscopy, you can see that many of the B cells are proliferating. What structure contains the germinal center and is responsible for somatic hypermutation and class switch recombination?
-
Primary follicle
-
Light zone
-
Dark zone
-
Mantle zone
-
Thymus
Answer C.
You perform an ELISA on a patient and find that she is deficient in AID. Which of the following processes is diminished in this patient?
-
Affinity maturation
-
V(D)J recombination
-
Tfh cell production
-
Central tolerance
-
Receptor editing
Answer C.
A 32-year-old man with no significant past medical history presents with a prolonged period of cough and repeated respiratory infections. As his physician, you order immunoglobulin levels to find the underlying cause of the recurrent infections. Test results show decreased IgA, IgG and plasma cells, but normal IgM. No one in his family has a history of immunodeficiencies and all seem to be relatively healthy. What is your diagnosis?
-
CVID
-
Selective IgA deficiency
-
Hyper-IgM syndrome
-
Hyper-IgA syndrome
-
SCID
Answer A.
B68-69: Tubular Reabsorption and Secretion III & IV
A 76 year old male patient presents to the clinic with edema in his lower extremities. He had been prescribed furosemide (loop diuretic) 6 months to combat this edema being caused by CHF. Which of the following explains this patients symptoms, despite being on a furosemide?
-
Increased number of ENaC are present causing increased Na+ reabsorption
-
Increased number of ROMK are present causing increased K+ secretion
-
Increased number of NCC are present causing increased Na+ reabsorption
-
The NCC in the DCT stop responding to Furosemide over time
-
The NKCC in the ATL stop responding to the Furosemide over time
Answer C.
Cortisol and aldosterone both display equal affinity to the mineralocorticoid receptor at the distal nephron. However, in healthy individuals cortisol actually has very little, if any, effect on renal reabsorption and secretion. Which of the following explains the reasoning for this?
-
Cortisol is inactivated by 11-βHSD2 to cortisone
-
Mg++ inhibits cortisol in the distal nephron
-
Cortisol is present in much lower quantities than aldosterone
-
Cortisol is completely reabsorbed before it reaches the distal nephron
-
Ca++ inhibits cortisol in the distal nephron
Answer A. Lecture #68-69: Tubular Reabsorption and Secretion III & IV
Your attending prescribes furosemide (loop diuretic) and a thiazide to a patient experiencing peripheral edema. She asks you what the purpose of prescribing these two diuretics together would be. What would be the most appropriate answer?
-
Furosemide causes hypercalcemia by indirectly inhibiting ROMK, whereas thiazides increase expression of TRPV5 causing hypocalcemia
-
Furosemide causes hypocalcemia by indirectly inhibiting ROMK, whereas thiazides increase expression of TRPV5 causing hypercalcemia
-
Furosemide causes hypocalcemia by indirectly inhibiting ROMK, whereas thiazides increase expression of TRPM6 causing hypercalcemia
-
Furosemide causes hypercalcemia by indirectly inhibiting ROMK, whereas thiazides increase expression of TRPM6 causing hypocalcemia
-
Furosemide causes hypocalcemia by directly inhibiting ROMK, whereas thiazides increase expression of TRPM6 causing hypercalcemia
Answer B.
A 32 year old female patient presents to the Emergency Department with nystagmus, convulsions, fatigue, muscle spasms, and numbness. Further testing reveals hypomagnesemia, most likely caused by chronic alcoholism. Which of the following could be a secondary effect of this hypomagnesemia?
-
Hypocalcemia
-
Hypokalemia
-
Hyponatremia
-
Hypercalcemia
-
Hyperkalemia
Answer B. Intracellular Mg2+ binds to and partially inactivates ROMK. Thus, Hypomagnesemia can result in refractory hypokalemia.
A patient has been given an EGF antagonist to aid in the treatment of colorectal cancer. Which of the following is potential side effect of this drug?
-
Hypocalcemia
-
Hyponatremia
-
Hypercalcemia
-
Hyperkalemia
-
Hypokalemia
Answer E. Lecture #68-69: Tubular Reabsorption and Secretion III & IV
A 56 year old female patient presents to the clinic complaining of polydipsia (extreme thirst), polyuria (excessive amounts of urine), and muscle weakness. The patient has a normal BGL. However, you suspect diabetes and prescribe ADH. However, one week later the patient returns and states the symptoms have not subsided. Which of the following is most likely leading to this patient’s symptoms?
-
Gestational diabetes insipidus
-
Central diabetes insipidus
-
Nephrogenic diabetes insipidus
-
Diabetes Mellitus Type I
-
Diabetes Mellitus Type II
Answer C.
Conn’s syndrome is a disease of the adrenal glands involving excess production of a hormone, called aldosterone. Based on this information, which of the following would NOT be a likely symptom of someone with this disease?
-
Hypokalemia
-
Acidic Urine
-
Hypertension
-
Hyponatremia
-
Alkalosis
Answer D. Excessive aldosterone upregulates ENaC, Na+K+ ATPase, NCC, ROMK, BK, H+ ATPase and AE1. Therefore it is involved in increases Na+ reabsorption and increased K+ secretion. Therefore, hypernatremia and hypokalemia are often commonly associated with an overproduction of aldosterone. Additionally, it upregulates H+ ATPase and AE1 associated with Type A cells. BEcause these channels are upregulated, more H+ is being secreted and therefore alkalosis and acidic urine will result. Hypernatremia is associated with increased water reabsorption and may result in hypertension. The only incorrect answer is hyponatremia.
Liddle’s syndrome is a genetic disorder inherited in an autosomal dominant manner that is characterized by a gain of function mutation in ENaC. Which of the following is a likely symptom of this disease?
-
Hyponatremia
-
Hypokalemia
-
Hypotension
-
Hypocalcemia
-
Acidosis
Answer B. An upregulation of ENac will cause excess K+ secretion via ROMK. Common symptoms of this disease include hypernatremia, hypokalemia, and hypertension.
Lecture #70-71: Renal Homeostasis I & II
A deficiency in aldosterone would result in which of the following?
-
Hyperosmotic overhydration
-
Isosmotic overhydration
-
Hyposmotic dehydration
-
Hyperosmotic dehydration
-
Isosmotic dehydration
Answer C. An aldosterone deficiency would lead to poor reabsorption of NaCl, leading to loss of NaCl in the urine. This would cause the osmolality of the plasma to decrease, so water would move to the ICF from the ECF.
The greater increase in production of AVP is caused by which of the following situations?
-
Decrease in blood volume
-
Increase in blood volume
-
Decrease in plasma osmolality
-
Increase in plasma osmolality
-
Decrease in colloidal osmolality
Answer A. A decrease in blood volume and an increase in plasma osmolality both cause the production of AVP to increase. The response to stimulus is greater in relation to decreased blood volume.
A patient with SIADH may experience a shift in compartmental fluid in which way?
-
An increase in both ECF and ICF
-
A decrease in both ECF and ICF
-
An increase in only ECF
-
An increase in only ICF
-
A decrease in only ECF
Answer: A. This condition, ADH will cause retention on water and salt, cause isotonic overhydration, and an expansion in both fluid compartments.
Which of these would be associated with the inability to concentrate urine?
-
Low water intake
-
SIADH syndrome
-
Low sodium diet
-
High protein diet
-
Urea deficiency
Answer: E. Urea is taken into the interstitial space at the inner medulla which pulls water with it. With low urea, the osmolality in the interstitium is decreased, and the water stays in the tubule.
ADH is synthesized in and secreted from the supraoptic nucleus and paraventricular nucleus in response to what factors?
-
A sudden drop in plasma osmolarity
-
A sudden increase in plasma volume
-
Increased thirst
-
Systemic vasoconstriction
-
Increase in EABV
Answer: C
A 54 year old male patient with a history of Diabetes Mellitus presents to the Emergency Department with a BGL of 630 mg/dL (normal is 90-110 mg/dL). Which of the following is true regarding this patient’s plasma osmolarity?
-
This patient will have hyposmotic plasma due to the excessive BGL pulling fluid into the ECF
-
This patient will have isosmotic since glucose does not play a major role in plasma osmolarity
-
This patient will have hyperosmotic plasma due to the excessive BGL
-
This patient will have hyperosmotic plasma due to the associated polyuria and loss of urea through the urine
-
This patient will have hyposmotic plasma due to the associated polyuria and loss of urea through the urine
Answer C.
A 35 year old female patient presents to the Emergency Department with severe burns cover 50% of her body. The immediate concern that your attending has is preventing infection and associated dehydration. Which of the following best describes the fluid change that this patient will encounter?
-
Hyperosmotic contraction
-
Hyposmotic contraction
-
Isosmotic contraction
-
Hyperosmotic expansion
-
Hyposmotic expansion
Answer C. Isosmotic contraction/dehydration can be caused by hemorrhage, exudation of plasma from burned skin or GI fluid loss due to N/V.
Which of the following examples would not lead to hyperosmotic contraction (dehydration)?
-
Diabetes mellitus
-
Diabetes insipidus
-
Alcoholism
-
Decreased water intake
-
Hemorrhage
Answer E.
The graph below represents total body water, ICF, and ECF volumes and osmolality. The solid line shows the osmolality and volume of a healthy individual. Which of the following best explains the dashed line?
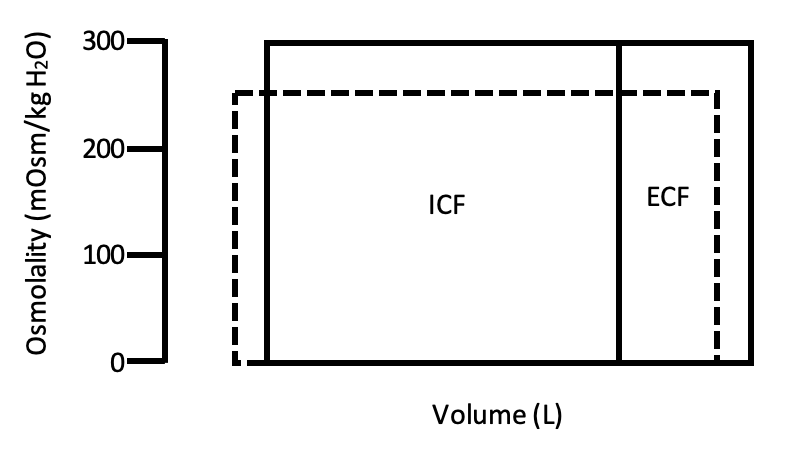
-
Hyposmotic contraction and aldosterone deficiency
-
Hyposmotic contraction and Diabetes insipidus
-
Isosmotic contraction and hemorrhage
-
Hyperosmotic contraction and Diabetes insipidus
-
hyperosmotic contraction and aldosterone deficiency
Answer A. Hyposmotic contraction is caused by a loss of NaCl. Aldosterone stimulates Na+ reabsorption and can therefore lead to this type of dehydration.
A patient presents to the Emergency Department after suffering from heat stroke and extreme dehydration. Unfortunately, you miscalculate and give the patient too much isotonic saline too fast. Which of the following graphs would most likely represent this situation? (The solid line represents a healthy individual and the dashed line represents this patient)
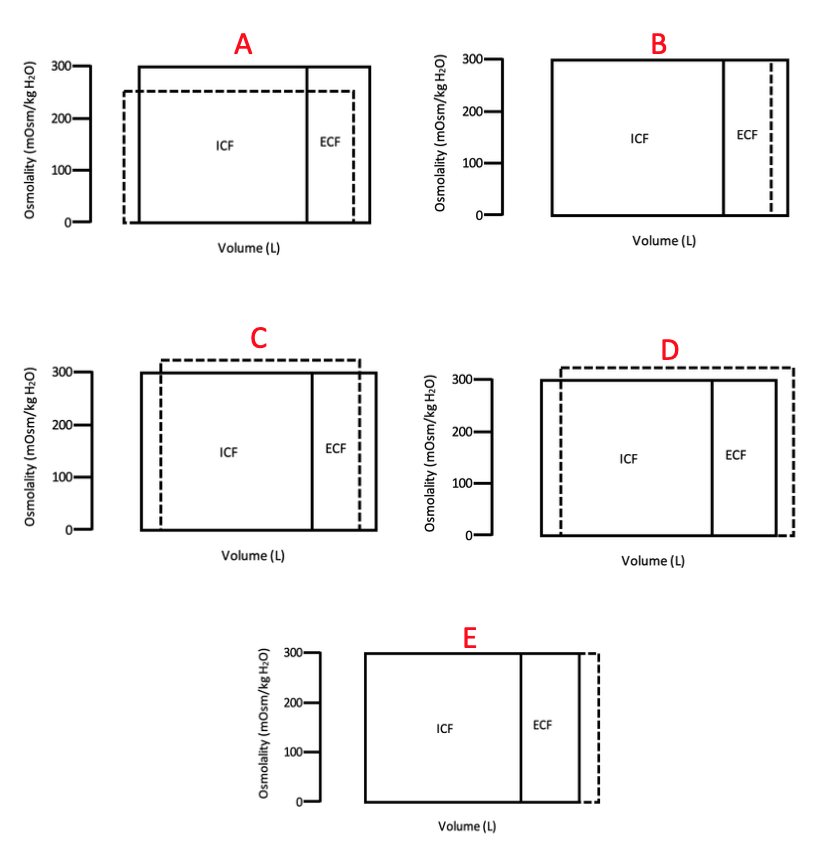
Answer E.
Inappropriate ADH secretion would likely lead to which of the following?
-
Isosmotic contraction
-
Hyperosmotic expansion
-
Hyperosmotic contraction
-
Hyposmotic expansion
-
Hyposmotic contraction
Answer D.
Which of the following are associated with decreased diuresis?
-
Alcohol consumption
-
Diabetes insipidus
-
Increased AVP
-
Diabetes mellitus
-
Release of ANP
Answer C. Alcohol, DI, ANP, and DM are all associated with increased diuresis. Alcohol and ANP work to suppress ADH/AVP. Diabetes insipidus can be caused by a deficiency in ADH or channels affected by ADH and Diabetes mellitus increases diuresis due to high filtrate osmolality caused by excessive BGL.
AVP (ADH) can be released in response to a number of different stimuli. Which of the following is associated with the greatest AVP release?
-
Minor loss in blood volume (-5%)
-
Major loss in blood volume (-20%)
-
Minor change in plasma osmolality (Goes from 285 mosm/kg H20 to 287 mosm/kg H2O)
-
Major change in plasma osmolality (Goes from 285 mosm/kg H20 to 300 mosm/kg H2O)
-
Major increase in ANP
Answer B. Blood volume loss results in the greatest AVP release once it is substantial enough. Osmolality changes work fast to cause ADH secretion, while blood volume loss works slower but has a much greater response.
Most people are more concerned about not drinking enough water. However, drinking too much water can also be dangerous. One of the side effects of overhydration is a urea deficiency. Which of the following would be associated with a urea deficiency?
-
Inability to concentrate the urine
-
Inability to dilute the urine
-
Nothing, urea is a toxin and therefore this specific side effect would not have any consequences
-
Inability to secrete ADH
-
Inability to secret ANP
Answer A.
Urine specific gravity is often used to provide rough estimates of the urine solute concentrations. Which of the following conditions may falsely suggest concentrated urine if evaluated using this test?
-
Diabetes insipidus
-
Diabetes mellitus
-
Inappropriate ADH
-
Aldosterone secreting adenoma
-
Excessive sweat production
Answer B. Glycosuria can falsely suggest concentrated urine because urine specific gravity measures the weight of solutes in a given volume and does not discriminate between glucose and other solutes that would indicate concentrated urine.
Medical researchers have found that estrogen birth control pills increase blood pressure in some women. This explains the reasoning behind why patients taking this contraception are at a higher risk for blood clots and ischemic stroke. Which of the following best describes the effect that oral contraceptives may have on renal reabsorption and secretion?
-
Estrogen works identically to Aldosterone to reabsorb sodium and water
-
Estrogen works identically to Progesterone to reabsorb sodium and water
-
Estrogen works identically to Aldosterone to secrete sodium and water
-
Estrogen works identically to Aldosterone to secrete sodium and reabsorb water
-
Estrogen works identically to Progesterone to secrete sodium and reabsorb water
Answer A.
You are on rotations in a family medicine clinic when a 72 year old male patient presents to the clinic with severe hypertension (206/110). The patient has been smoking ½ pack a day for the last 30 years and your attending believes he has developed atherosclerosis. Which of the following is a potential mechanism accounting for this patient’s high blood pressure?
-
Renal artery stenosis caused by atherosclerosis could lead to excessive Renin production
An aldosterone-producing adenoma is a noncancerous (benign) tumor that develops in an adrenal gland and can cause a condition known as primary hyperaldosteronism. However, it doesn’t usually result in chronic edema formation of frank hypernatremia. Which of the following best explains the mechanism behind this compensation?
-
Mineralocorticoid escape results by stretching of the atria and release of ANP
-
Mineralocorticoid escape results by stretching of the atria and release of ADH
-
Mineralocorticoid escape results by stretching of the atria and release of Angiotensin II
-
Mineralocorticoid escape results by stretching of the atria and release of Progesterone
-
Large amounts of aldosterone cause diuresis by degrading urea
Answer A.
A sudden increase in blood pressure can cause diuresis through which of the following methods?
-
Pressure natriuresis causes backflow of Na+ into the filtrate by widening gap junctions
-
Increased blood pressure can decrease activity of Na+K+ ATPase
-
Increased blood pressure can decrease activity of NHE3
-
A & B
-
A, B, & C
Answer E. Note that inhibition of NHE3 can result in acidosis.
Which of the following could be given to a patient in order to correct hyperkalemia?
-
NaHCO3
-
Insulin
-
Epinephrine
-
A & B
-
A, B & C
Answer E.
A patient presents to the clinic with hyperparathyroidism resulting in excessive PTH production. If urinalysis is conducted, which of the following is likely to be found in excess?
-
Calcium
-
Sodium
-
Phosphate
-
Potassium
-
Glucose
Answer C.
Lecture #72: Metabolism of the Kidney/Renal Functional Measures
Which of the following is true regarding the concentration of glutamine and Glucose in the Renal artery (RA) compared to the Renal Vein (RV)?
-
RA Glucose > RV Glucose
-
RA Glucose < RV Glucose
-
RA Glutamine < RV Glutamine
-
RA Glutamine > RV Glutamine
-
RA Glutamine = RV Glutamine
Answer D.
Which of the following most accurately explains the renal metabolism?
-
Medullary glycolysis produces mainly lactate that can be used for cortical gluconeogenesis
-
Cortical glycolysis produces mainly lactate that can be used for medullary gluconeogenesis
-
Cortical glycolysis produces mainly glutamine that can be used for medullary gluconeogenesis
-
Medullary glycolysis produces mainly glutamine that can be used for cortical gluconeogenesis
-
Medullary glycolysis produces mainly alanine that can be used for cortical gluconeogenesis
Answer A.
Diabetic ketoacidosis (DKA) is associated with all of the following EXCEPT?
-
Increase in renal gluconeogenesis
-
Decrease in hepatic gluconeogenesis
-
Polyuria
-
Dehydration
-
Increased glucagon
Answer E.
It is believed that ammonia can be reabsorbed through all of the following methods EXCEPT?
-
NH3 diffusion
-
NH4+ transport via NHE3 in the PCT
-
NH4+ transport via NKCC2 in the TAL
-
NH4+ transport via ROMK in the TAL
-
Diffusion by Rhbg and Rhcg
Answer D.
A patient on Invokana has a plasma glucose level 100 mg/dL, inulin clearance of 130 mL/min, urine production of 2 mL/min and glucose concentration in urine 900 mg/dl. Which of the following is closest to this patient’s transport maximum of glucose?
-
112 mg/min
-
1120 mg/min
-
11200 mg/min
-
1170 mg/min
-
11700 mg/min
Answer A.
Lecture #73: Renal Acid Base Regulation
The following graph depicts the pH of a urine sample as it is titrated with Sodium hydroxide (NaOH). Based on the graph, which of the following values is closest to the amount of titratable acids in this sample of urine?
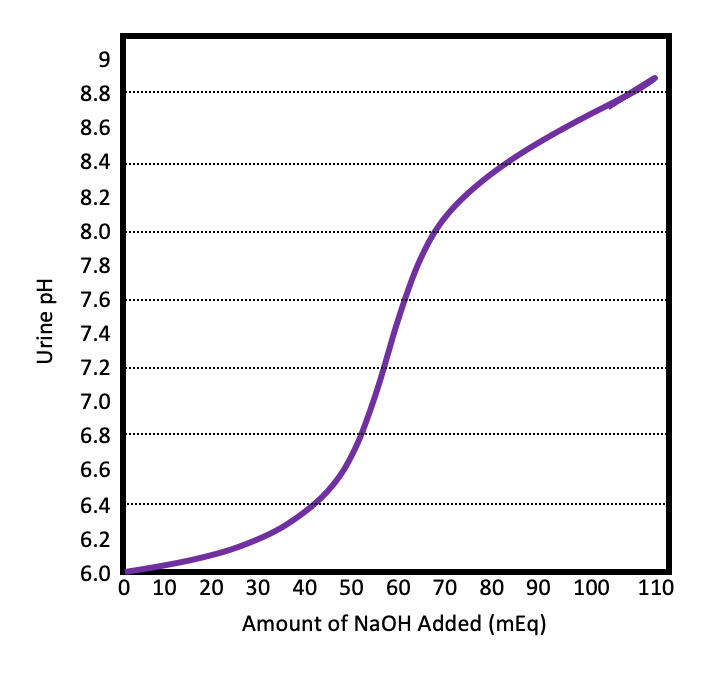
-
30 mEq
-
40 mEq
-
60 mEq
-
80 mEq
-
90 mEq
Answer C. The amount of titratable acids should be equal to the amount of NaOH added to the urine sample at a pH of 7.4 (physiologic). In this case, the best answer is 60 mmol.
Which of the following pH values will be associated with the largest amount of phosphate in the monovalent form (HPO42-)?
-
5.4
-
6.2
-
6.8
-
7.4
-
8.4
Answer E. The pKa is 6.8 so any pH above this will have >50% in monovalent form. 8.4 is the greatest pH so it will have the largest amount of HPO42-.
Calculate the net renal acid excretion from the following values.
Titratable acid: 26 mEq/d
Urinary ammonia: 50 mEq/d
Glucose: 20 mEq/d
Urinary HCO3-: 1 mEq/d
pH: 6.4
-
69 mEq/d
-
75 mEq/d
-
46 mEq/d
-
97 mEq/d
-
51 mEq/d
Answer B.
Lecture #77: Regulation of the Immune Response
Activation-induced cell death is a method of controlling lymphocyte expansion than, when defective, results in autoimmune lymphoproliferative syndrome. What would you expect to occur in a healthy person during AICD?
-
Expression of high affinity receptors for T cell growth factor
-
Fratricidal apoptosis by FasL-Fas interactions
-
Activation of Treg cells and subsequent secretion of IL-10 and TGFβ
-
Interactions of protein B7 and CTLA-4
-
Blockade of the PD1 checkpoint
Answer B
In a patient with a severe autoimmune deficiency due to a failure of negative selection in thymus, you would expect to find a deficiency in which critical player in the regulation of the immune response?
-
FasL
-
CTLA-4
-
PD-1
-
FOXP3
-
AIRE
Answer E.
B78: Microbial Activation of the Immune Response
A UFAS biology student comes in to the emergency department with a sore throat, fever, and a red rash spreading over his back. While getting the patient’s HPI, he tells you that after a recent hike through Devil’s Den, he had to remove several ticks from himself and is worried he may have a serious infection. Which natural immunity effector cell is playing a vital role in fighting of this suspected infection, which you believe to be caused by rickettsia?
-
Eosinophils
-
Neutrophils
-
Natural killer cells
-
DCs
-
Basophils
Answer: C. Rickettsia is an obligate intracellular parasite, and so NK cells will play a major role in the natural immune response to this pathogen.
Lecture #79: Hypersensitivities
A 53 year old male patient presents to the Emergency Department following a suspected anaphylactic reaction. The patient has been treated and mentions that the reaction directly followed the accidental ingestion of peanut oil. Which of the following proteins is most likely responsible for this reaction?
-
ARA h 1
-
ARA h 2
-
ARA h 3
-
ARA h 8
-
ARA h 9
Answer D.
A 5 year old female patient presents to the Emergency Department following a suspected anaphylactic reaction. The patient has been treated and the mother mentions that the reaction directly followed the ingestion of peanuts. Which of the following proteins is most likely responsible for this reaction?
-
ARA h 1
-
ARA h 2
-
ARA h 3
-
ARA h 8
-
ARA h 9
Answer B.
A patient is rushed to the hospital via ambulance after she was bitten by a large copperhead. On arrival, she is given horse antiserum against the snake’s venom and develops serum sickness. This reaction is mediated by which hypersensitivity mechanism?
-
Th17 response
-
Th1 response
-
Anti-DNA antibodies
-
Conglomeration of immune complexes
-
IgE antibody activity
Answer: D. Serum sickness is a Type III hypersensitivity.
Which of the following is TRUE regarding the relationship between potassium and renal pH regulation?
-
Hypokalemia will cause an extracellular shift of potassium and an intracellular shift of hydrogen ions resulting in metabolic acidosis
-
Hyperkalemia will cause an extracellular shift of potassium and an intracellular shift of hydrogen ions resulting in metabolic acidosis
-
Hypokalemia will cause an extracellular shift of potassium and an intracellular shift of hydrogen ions resulting in metabolic alkalosis
-
Hyperkalemia will cause an extracellular shift of potassium and an intracellular shift of hydrogen ions resulting in metabolic alkalosis
-
Hypokalemia will cause an extracellular shift of hydrogen ions and an intracellular shift of potassium ions resulting in metabolic acidosis
Answer C.
B80: Tolerance and Autoimmunity
You are doing diagnostic testing on a patient, including a test for Anti-AchR. Anti-AchR stabilizes the postsynaptic membrane and prevents depolarization, often leading to diplopia and ptosis. The presence of Anti-AchR antibodies would be indicative of which autoimmune disease?
-
Myasthenia gravis
-
Graves’ disease
-
Goodpasture syndrome
-
Systemic lupus erythematous syndrome
-
Addison’s disease
Answer A.
Testing for rheumatoid arthritis often includes C-reactive protein quantification, but that is not enough to give a definitive diagnosis. What other test result would you need to confirm your diagnosis?
-
Elevated melanocyte stimulating hormone (MSH)
-
Elevated thyroid peroxidase
-
Elevated thyroid stimulating hormone (TSH)
-
anti-cyclic citrullinated peptide (anti-CCP) antibodies
-
HLA-B27
Answer D.
Which of the following is a type IV hypersensitivity?
-
Systemic lupus erythamatous
-
Myasthenia gravis
-
Graves’ disease
-
Diabetes mellitus
-
Goodpasture syndrome
Answer D.
A patient presents with complaints of coughing up blood and painful urination. You run some tests and find that he has an increased number of anti-type IV collagen IgG. What is your diagnosis?
-
Hashimoto’s thyroiditis
-
Graves’ disease
-
Goodpasture syndrome
-
Multiple sclerosis
-
Myasthenia gravis
Answer C.
Citrullinated proteins – RA
SLE – anti-DNA antibodies
Myasthenia gravis – anti-AchR antibodies
Anti-collagen IV antibodies – Goodpasture syndrome – type II hypersensitivity
B81: Adaptation & Cell Death I: Cellular Response to Injury
During pregnancy, the uterus must increase in size to accommodate the fetus and placenta. At full term, the uterus can weigh as much as 15 times its weight prior to conception. What mechanism is responsible for this drastic increase in size?
-
Physiologic hypertrophy
-
Pathologic atrophy
-
Physiologic hyperplasia
-
Pathologic hyperplasia
-
Physiologic metaplasia
Answer A.
What would you observe following damage to the mitochondrial membrane?
-
Decreased extracellular calcium
-
Increased cytosolic calcium
-
Increased ATP production
-
Increased release of RNAses
-
Decreased production of proteases
Answer B.
85: Adaptation and Cell Death II: Cell Death
B86: Environmental Mechanisms I: Cell Injury
B87: Environmental Mechanisms II: Physical Injury