- A 72 year old patient presents to the clinic complaining of shortness of breath, and fatigue. He is an avid smoker (1 pack a day for the last 30 years). He denies alcohol use. Upon examination, you note a systolic murmur heard best along the right eternal border in the second intercostal space. Which of the following are you most likely to see on an ECG (lead II)?
- Peaked P
- Bifid M shaped P wave
- ST Depression
- ST Elevation
- Absent P waves
You are concerned that a patient might have right atrial enlargement due to ongoing COPD. Which lead are you primarily going to analyze to determine if your suspicion is true?
- I
- III
- aVR
- V2
- V1
Which of the following is the most likely cause of right ventricular hypertrophy?
- Aortic Stenosis
- Systemic Hypertension
- Atrial septal defect
- Aortic Regurgitation
- Coarctation of the aorta
Which of the following is NOT a primary symptom of a right-to-left shunt?
- Polycythemia
- Clubbing of fingertips
- Cyanosis
- Hypoxemia
- Pulmonary hypertension
You are on rounds in OB-GYN when your attending calls you out to answer a question. She explains that the patient, a 2 week old female infant, is undergoing treatment with Indomethacin. Indomethacin is drug used to lower PGE2 levels. She also states that the patient is being treated for congenital Rubella. She asks you which congenital heart defect they are trying to correct with this medication. What is your answer?
- Atrial Septal Defect
- Ventricular Septal Defect
- Tetralogy of Fallot
- Patent Ductus Arteriosus
- Patent Foramen Ovale
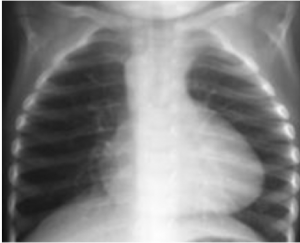
You are on rotations in OB-GYN where you are assisting in the delivery of a 3 week premature infant. Upon delivery, the infant has an APGAR of 6 and is displaying early cyanosis. Initial examination reveals a systolic murmur heard along the left sternal border in the 2nd intercostal space. After measures are taken to stabilize the infant, your attending orders a chest x-ray that is shown below. Which of the following is most likely the cause for the infant’s symptoms?

- Atrial Septal Defect
- Ventricular Septal Defect
- Tetralogy of Fallot
- Patent Ductus Arteriosus
- Patent Foramen Ovale
Which of the following is a result of severe congenital aortic stenosis?
- Left Ventricular Hypertrophy
- Left Ventricular Hypoplasia
- Right Ventricular Hypertrophy
- Right Ventricular Hypoplasia
- Ventricular Septal Defect
A 55 year old male patient presents to the clinic with a diastolic murmur best heard in the 5th intercostal space along the mid-clavicular line. Which of the following is most likely to be found in this patient’s history?
- Long History of Smoking
- Congenital Heart Defect
- Rheumatic Fever as a child
- Marfan Syndrome
- Familial History of MI
Dilated cardiomyopathy (DCM) shows progressive cardiac dilation with poor contractile, resulting in systolic dysfunction. A positive test for which of the following would support a suspected diagnosis of DCM in a patient also denying alcohol use?
- Coxsackie A
- Streptococcus pyogenes
- Staphylococcus aureus
- Streptococcus viridans
- Parvovirus B19
Which of the following occurs first in cardiac ischemia?
- Chest Pain
- Electrical Transit Abnormalities
- Regional Systolic Dysfunction
- Diastolic Dysfunction
- Myocardial necrosis
What is the number one cause of cardiac ischemia?
- Prinzmetal’s angina
- Arterial thrombi
- Atherosclerosis
- Coronary emboli
- Congenital abnormalities
Which of the following is NOT a component of atherosclerotic plaques?
- Subintimal collections of fat
- Smooth muscle cells
- Fibroblasts
- Intercellular matrix
- Elastic connective tissue
Which of the following post MI complications is likely to need a permanent pacemaker?
- Complete AV block due to inferior infarction
- Complete AV block due to anterior infarction
- Second degree AV block
- Atrial Flutter
- Supraventricular Arrhythmia
A patient presents to the Emergency Department with symptoms of an acute MI. Following treatment and examination, your attending asks you what the Killip classification of this patient is. You noted an S3 heart sound and rales in approximately 75% of the lung field. What is your answer?
- Class I
- Class II
- Class III
- Class IV
- Class V
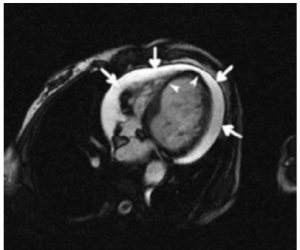
A 63 year old male patient presents to the clinic complaining of chest pain. He tells you that he is worried he is “having a heart attack again.” He was released from the Emergency Department only 2 weeks prior for an acute MI. Upon examination, you note a fever and friction rub. You perform a CT, which is shown below. What’s the diagnosis?
- Cardiogenic shock
- Ventricular aneurysm
- Ventricular septal rupture
- Dressler’s Syndrome
- Papillary muscle dysfunction
Which of the following is NOT a component of ACS management?
- Heparin
- Nitroglycerin
- ACE inhibitors
- Clopidogrel
- Calcium channel blockers
Analyze the ECG below. Which of the following best describes your diagnosis?
- First Degree Heart Block
- Mobitz Type-I
- Mobitz Type-II
- 2:1 Block
- 3rd Degree Heart Block
Analyze the rhythm strip below (Lead II). Which of the following is your diagnosis?
- Normal Sinus Rhythm
- Sinus Bradycardia
- First Degree Heart Block
- Second Degree Heart Block
- Torsades de Pointe
A patient comes in with complaints of heart palpitations feeling tired for the last several days. You order an ECG with the following results. With the patient’s history positive for asthma, which of the following medications would be best to correct the abnormality seen on ECG?
- Amiodarone
- Propafenone
- Mexiletine
- Lidocaine
- Flecainide
After a medical student collapsed due to finally getting back an exam score, they were taken to a nearby hospital, and required cardioversion to fix a dangerous arrhythmia. Within a few days of discharge, they began to experience severe headaches, nausea, and vomiting. They returned to the clinic with these symptoms along with complaints of a high-pitched ringing sound. Which drug was likely given to them that could have caused these symptoms?
- Quinidine
- Mexiletine
- Propafenone
- Esmolol
- Digoxin
Which of the following scenarios would encourage you to perform an Echo in a newborn patient (24-48 hours of age)?
- POX of 90% on the right hand and 89% on left hand
- POX of 93% on right hand and 92% on the left hand
- POX of 90% on left root
- POX of 90% on the left foot and 95% on right hand
- None of the above would indicate the need for an echo
You are performing a physical exam on a newborn patient. The patient is acyanotic but you notice a wide fixed splitting of S1-S2 and systolic murmur at the left 3rd intercostal space. You suspect an atrial septal defect, and perform an echo. You note an ASD on the inferior aspect of the interatrial wall, proximal to the endocardial cushion. Which of the following comorbidities is this patient likely to have?
- Down Syndrome
- Marfan Syndrome
- Congenital Rubella
- Rheumatic Fever
- Ventricular Septal Defect
You are on rotations in OB-GYN where you help to deliver a newborn baby girl. The patient is generally healthy in appearance, with an APGAR of 9 (some distal extremity cyanosis is present). Your attending assures you that this is relatively normal for most newborns. Heart sounds are normal. PMI is located in the 4th intercostal space along the left mid clavicular line and lung sounds are heard in all quadrants with no wheezing or crackles. However, you note that the patient is experiencing inspiratory dyspnea. What is the most likely diagnosis?
- Coarctation of the aorta
- Aortic Stenosis
- Ventricular Septal Defect
- Tetralogy of Fallot
- Double Aortic Arch
You are on rotations in OB-GYN when you help to deliver a newborn baby boy via cesarean section. The baby has an APGAR of 7 with severe cyanosis, weak cry, and low activity. Appropriate measures are taken to stabilize the infant and the nurse begins ventilation via BVM. Lab results show a substantial PaO2 difference between the right radial and umbilical arteries. You perform an echo which reveals interventricular flattening. Which of the following is a suitable treatment for this infant?
- Aspirin administration
- Blalock-Taussig shunt
- PGE2 administration
- Beta Blockers
- There is no treatment available
Which of the following is a common demographic for children diagnosed with Kawasaki Disease?
- Females
- Caucausin
- Hispanic
- Pacific Islander
- Black
A 2 year old male patient presents to the clinic. The mother explains that the child has weird rash on his tongue and swelling in his hands and feel. Upon examination you also notice non-suppurative conjunctivitis and desquamation in the fingertips. The child has a fever of 101 ºF and an enlarged right anterior cervical lymph node. Which of the following lab results are you likely to find?
- Increased LDH
- Decreased ESR and CRP
- Markedly elevated Platelet count
- Decreased WBCs
- Increased RBCs
Which of the following is NOT part of the major Jones criteria?
- Migratory arthritis
- Carditis
- Erythema marginatum
- Subcutaneous nodules
- Fever
A 25 year old female patient presents to the clinic with a decreased appetite, sudden weight loss, abdominal pain, excessive fatigue, and fever. She is also complaining heavily of a painful, pruritic, nodular like rash located on her legs that she believes to be unrelated. Her history is positive for Hepatitis B and Diabetes Mellitus Type I. Which of the following is likely affecting this patient?
- Giant Cell Arteritis
- Granulomatosis with Polyangiitis
- Eosinophilic Granulomatosis with Polyangiitis
- Polyarteritis Nodosa
- Kawasaki Disease
A positive test for c-ANCA could confirm which of the following diagnoses?
- Giant Cell Arteritis
- Granulomatosis with Polyangiitis
- Eosinophilic Granulomatosis with Polyangiitis
- Microscopic Polyangiitis
- Kawasaki Disease
Which of the following can help you confirm a diagnosis of a tumor of endothelial origin?
- p-ANCA
- c-ANCA
- CD31
- CD55
- HBsAg
A 32 year old male patient presents to the clinic with concerning cutaneous red-purple plaques on his foot. He has a history of HIV. Which of the following are likely to be positive?
- p-ANCA
- CD55
- CD31
- HBsAg
- HHV-8 Ag
You are seeing a 23 year old man in the ED who is complaining of sudden onset severe substernal pain that has begun to radiate to his back which began at rest. His respiratory rate is 28 and he is having difficulty staying alert. Initial labs show normal troponin.What test would give you the best chance of immediately confirming your diagnosis?
- TEE
- Abdominal CT with contrast
- ECG
- Renal Angiography
- CXR
A 58 year old male patient presents to the clinic for a health exam. He is feeling generally healthy and has no complaints besides his typical symptoms of osteoarthritis in his hands. History is positive for a 30 pack year. You are palpating his abdomen when you feel a large, periumbilical, pulsatile mass. You order imaging which shows a 3cm AAA, confirming your diagnosis. Which of the following is TRUE regarding this individual?
- Surgery is not indicated at this time since the patient’s risk for rupture is virtually non existent
- This patient needs timely surgery to prevent imminent rupture
- This patient has an 11% annual risk of rupture
- This patient has a 25% annual risk of rupture
- This patient has a 1% annual risk of rupture
Which of the following is INCORRECT regarding aortic aneurysms and dissections?
- Hypertension is the major risk factor for ascending aortic aneurysm
- Marfan syndrome is often associated with aortic dissections
- Ehlers Danlos is often associated with aortic dissections
- Atherosclerosis is the major risk factor for abdominal aortic aneurysms
- Infective endocarditis is highly correlated with aortic dissections
One of your patients with a history of endocarditis has called you to ask for prophylactic antibiotics preceding a root canal in the near future. He is positive for allergies to beta lactam antibiotics and has difficulty with some medications due to age and progressing Parkinson’s disease. What would be an appropriate prescription for this patient?
- Amoxicillin PO 1h before procedure
- Ampicillin 2g IV 1hr before procedure
- Clindamycin 600mg IV 1hr before procedure
- Cephalexin 2g PO 1hr before procedure
- Clarithromycin 500mg PO 1hr before procedure
Which symptom, when paired with the presence of carditis and evidence of GAS infection, is NOT sufficient for a diagnosis of ARF?
- Chorea
- Elevated ESR and CRP
- Subcutaneous nodules
- Polyarthritis
- Chorea
A 56 year old man who you have seen for years comes in for a wellness check. He has a blood pressure of 140/80 and has been on medication for his HTN for years. For the past few weeks he has been complaining of difficulty with urination, with a stream that starts and stops. Following your suspicions, you receive a positive blood test for a specific tumor biomarker. What drug could you replace his current HTN medication to help with his newly onset symptoms?
- Captopril
- Losartan
- Methyldopa
- Nifedipine
- Doxazosin
A patient comes into the clinic for a follow-up 7 days after being discharged from the hospital following an acute myocardial infarction. The patient is complaining of feeling tired throughout the day and being short of breath when they exert themselves. They have also been unable to perform with their partner. ROS is negative for arthralgia or muscle pain. Which of the following medications is most likely the cause of their symptoms?
- Lisinopril
- Atenalol
- Clopdigrel
- Atorvastatin
- Verapamil
You are attempting to treat a patient with hypertension who has a history of asthma. Which of the following drugs would be most appropriate to prescribe initially?
- Atenolol
- Amiodarone
- Captopril
- Aliskiren
- Clonidine
Which of the following drugs is NOT associated with torsades de pointe as a side effect?
- Disopyramide
- Quinidine
- Procainamide
- Dofetilide
- Sotalol
Which of the following drugs is used to treat bradycardia?
- Adenosine
- Digoxin
- Atropine
- Magnesium Sulfate
- Captopril
A 75 year old male patient presents to the clinic for a wellness check. He has a history of diabetes mellitus that he states has been well controlled with diet and use of Metformin. Last time you saw him, you diagnosed him with HTN which you prescribed Lisinopril to control. Although this patient has been taking his medications religiously, his blood pressure is still reading slightly high at 146/88. You decide to prescribe an adjuvant drug. Which drug would you want to AVOID giving to this patient?
- Valsartan
- Losartan
- Methyldopa
- HCTZ
- Aliskiren
A 75 year old male patient presents to the clinic for a wellness check. He has a history of diabetes mellitus that he states has been well controlled with diet and use of Metformin. Last time you saw him, you diagnosed him with HTN which you prescribed Lisinopril to control. While his blood pressure has been well controlled since, he is complaining of a persistent cough. Which of the following drugs would you replace with lisinopril to reduce this side effect?
- Losartan
- Methyldopa
- HCTZ
- Aliskiren
- Fosinopril
- A 58 year old female presents to the ER complaining of general fatigue/weakness, numbness, and nausea/vomiting. History reveals a history of hypertension, which has been controlled with a medication she can’t seem to remember the name of. She notes that she had been having a history of painful leg cramps a couple months back. Her friend recommended taking potassium supplements over the counter to help. Based on this information, which of the following drugs is this patient most likely taking to control her hypertension?
- Methyldopa
- HCTZ
- Aliskiren
- Candesartan
- Clonidine
- A patient with Pheochromocytoma would most benefit from which combination of drugs to control HTN?
- Phenoxybenzamine and Procainamide
- Phenoxybenzamine and Propranolol
- Phenoxybenzamine and Doxazosin
- Procainamide and Doxazosin
- Procainamide and Prozosin
- Which of the following drugs are contraindicated with the administration of Nitroglycerin?
- Aspirin
- Morphine
- Viagra
- Losartan
- Cholestyramine
- Which drug is best for the treatment of Type III hyperlipoproteinemia?
- Gemfibrozil
- Ezetimibe
- Alirocumab
- Lomitapide
- Mipomersen
- A 63 year old man is at dinner. When he is chewing his food, he begins to feel like he has a headache. He arrives at the clinic and your workup shows an elevated ESR. Your biopsy shows the following:
What is your diagnosis?- Giant Cell (Temporal) arteritis
- Takayasu arteritis
- Kawasaki Disease
- Polyarteritis Nodosa
- Churg-Strauss Syndrome
- Which of the following serology components is found in a 37-year-old with polyarteritis nodosa?
- Heterophile antibodies
- Positive dsDNA antibodies
- Positive p-ANCA
- Hepatitis B surface antigens
- Antibodies to basement membrane
- A 62 year old man presents complaining of shortness of breath and mild chest pain when walking up the stairs at his apartment for the past 2 months. He does not have any significant prior medical history. On exam, you note a 2/6 holosystolic murmur at the 5th intercostal space to the left of the sternum. Which of the following is the correct murmur.
- Mitral Stenosis
- Mitral Regurgitation
- Aortic Stenosis
- Aortic Regurgitation
- Mixed Mitral Valve Disease
- A 24 year old female with a history of hypertension presents with symptoms of hypokalemia. She is currently taking an ACE inhibitor for hypertension control. Following laboratory testing, you notice her aldosterone is elevated and she is hypokalemic. You discover the underlying cause of they hyperaldosterinism is most likely due to an adrenal gland tumor. Which drug will you administer to this patient?
- Acebutolol
- Spironolocatone
- Valsartan
- Aliskiren
- Lisinopril
- Which of the following is TRUE regarding Cysticercosis?
- You can only get it from eating undercooked pork
- It’s caused by T. sanginata.
- It results in elephantiasis
- Its a relatively asymptomatic disease
- It can cause cysts in the brain