
Included Content
1. Which segment of an immunoglobulin is responsible for determining the class of the antibody?
-
V segment of the light chain
-
V segment of the heavy chain
-
D segment of the heavy chain
-
C segment of the light chain
-
C segment of the heavy chain
2. Which of the following segments are found only in the heavy chain of an immunoglobulin?
-
C segment
-
D segment
-
G segment
-
J segment
-
V segment
3. A patient seen in the ED presents with an acute infection. Which antibody class is likely to be elevated in an acute infection?
-
IgG
-
IgA
-
IgM
-
IgE
-
IgD
4. At the beginning of the year you kept getting constant emails from CastleBranch asking about titer levels and other stuff you probably found irrelevant. What type of antibody are titers most likely checking for?
-
IgG
-
IgA
-
IgM
-
IgE
-
IgD
5. When you finally have time to go home for a weekend after the hell weeks ARCOM scheduling puts you through, you decide to go hiking with your best friend from high school. While hiking your friend’s leg begins to become incredibly inflamed after brushing up against some weird green thing called “a plant”. You, being the little nerd that you are, decided to tell them what antibody is likely causing the inflammatory reaction instead of doing literally anything useful. What type of antibody has the shortest half-life and is likely responsible for this reaction?
-
IgG
-
IgA
-
IgM
-
IgE
-
IgD
6. While taking a break you start to scroll on facebook and notice all of your non-med school friends doing things like buying houses, traveling, and having kids. You can’t stop thinking about school and about which antibodies are conveyed from mother to child as a natural passive immunity. Which of the antibody classes are transferred from mom to baby in the last 1-2 months PRIOR to birth?
-
IgG
-
IgA
-
IgM
-
IgE
-
IgD
7. While taking a break you start to scroll on facebook and notice all of your non-med school friends doing things like buying houses, traveling, and having kids. You can’t stop thinking about school and about which antibodies are conveyed from mother to child as a natural passive immunity. Which of the antibody classes are transferred from mom to baby POST birth?
-
IgG
-
IgA
-
IgM
-
IgE
-
IgD
8. Which of the following antibody classes is found circulating as a pentamer or “star burst” and is known to be the best at activating the classical complement pathway?
-
IgG
-
IgA
-
IgM
-
IgE
-
IgD
9. Which of the following antibodies are produced almost exclusively in MALTs (Mucosa Associated Lymphoid Tissues) due to the high concentration of TGF-Beta and thus more likely to be secreted across mucosal membranes?
-
IgG
-
IgA
-
IgM
-
IgE
-
IgD
10. A double null mutation in the gene that produces Poly-Ig-Receptor (PIgR), would cause which of the following to occur?
-
Lack of IgA in both the blood and external surfaces
-
Lack of IgM in both the blood and external surfaces
-
Lack of IgA in the blood but not the external surfaces
-
Lack of IgM in the blood but not the external surfaces
-
Lack of IgA in the external surfaces but not in the blood
11. Which of the following aspects of a vaccination would improve alimentary (nasal and GI) immunity such as the poliomyelitis vaccination by Sabin?
-
Intravenous administration
-
Intramuscular administration
-
Oral administration
-
An inactivated virus
-
A vaccine composed of cytoplasmic proteins from a bacterium
12. Which of the following antibody functions is essential for the purpose of vaccinations against certain viruses?
-
Neutralization
-
Opsonization
-
Degranulation
-
Phagocytosis
-
Complement dependant cell cytotoxicity (CDCC)
13. Which class of antibody is most important for activating antibody dependent cell cytotoxicity (ADCC) with NK cells?
-
IgG
-
IgA
-
IgM
-
IgE
-
IgD
14. Which of the following lymphatic cancers is associated with multinucleated Reed-Sternberg cells and EBV?
-
Hodgkin’s Disease
-
Acute Lymphoblastic Leukemia
-
Chronic Lymphoblastic Leukemia
-
Multiple myeloma
-
Non-Hodgkin’s lymphoma
15. A patient present to the clinic with a genetic abnormality that results in a dysfunctional D segment, which variable region is altered?
-
VL
-
VH
-
CL
-
CH
-
CS
16. Which of the following lengths of base pairs is accepted by the recombination signal sequences?
-
17
-
22
-
20
-
10
-
12
17. A patient presents to the clinic with increased levels of TREC. A deficiency/defect in which of the following combinatorial diversity aspects results in the diagnosis of RS-SCID?
-
RAG1/2
-
NHEJ
-
Exonuclease Activity
-
TdT activity
-
DNApol µ & λ
18. What is analogous to the SLC and joins rearranged ꞵ-chain to form pre-TCR?
-
pre-TCRꞵ
-
Rearranged ɑ-chain
-
pre-TCRɑ
-
pre-SLC
-
Rearranged κ-chain
19. In regards to serum free light chain ratio, which of the following statements is true?
-
Half-life of FLC is normally 6-8 hours
-
Κ:λ is less sensitive than FLV concentration
-
>90% of patients with MM or AL have normal Κ:λ
-
Normal κ:λ reference range is .26 – 1.65
-
Κ:λ cannot be used for prognostication
20. Which of the following is NOT a true of AID (Activation-induced deaminase)?
-
Inserts cytosine to uracil mutations
-
Deficiency causes absent Ig CSR
-
Deficiency causes lack of Ig SHM
-
Deficiency causes lymph node hypoplasia
-
Stimulates switch regions between different C segment
Session 73 – T Cell Development
22.Presence of which types of cells would enable one to distinguish features of DiGeorge syndrome versus SCID ?
-
B cells
-
T helper cells
-
NK cells
-
Macrophages
-
Dendritic cells
23. Which cells do not express MHC class I and II molecules?
-
B cells
-
Thymus epithelial cells
-
Neutrophils
-
Macrophages
-
Dendritic cells
24. Negative selection is expressed by ___ in the ___?
-
cTEC; cortex
-
cTEC; medulla
-
mTEC; cortex
-
mTEC; medulla
-
mTEC; paracortex
25. Where could a cognate antigen be found?
-
Capsule of thymus
-
Medulla of thymus
-
PALS of spleen
-
Bone marrow
-
liver
26. Which is not a component of the V/D/J rearrangement of developing thymocytes?
-
CD3
-
RAG
-
TdT
-
AIRE
-
pre-TCR alpha
Session 74 – Transplant Immunology
27. Since the introduction of immunosuppressive reagents, what has become most critical in determining a viable solid organ transplant?
-
HLA Matching
-
Tissue Rejection
-
Anti-Donor Antibodies
-
Donor CTLs
-
Xenogeneic Antibodies
28. Following an organ transplant, the antibodies already present in your patient begin to activate complements to attack the organ tissue. What category of rejection is this?
-
Acute
-
Chronic
-
Hypochronic
-
Hyperacute
-
Hypoacute
29. Due to the medications prescribed to a patient following a solid organ transplant, these patients are at a higher risk for…?
-
Rejection of future transplants
-
Future Infections
-
Future rejection of current transplants
-
More necessary organ transplants
-
Medication sensitivity
30. What is the purpose of the first step in Hematopoietic Stem Cell Transplantation?
-
To find donor HSCs
-
To find HSCs without mature T-Cells
-
To match HLAs
-
To limit the rejection of the graft
-
To Increase the likelihood of GSVD
31. Cyclosporines, Rapamycin, Basiliximab, and high doses of corticosteroids all affect what immunological agent?
-
T-Cells
-
B-Cells
-
APCs
-
DCs
-
Antibodies
Session 75 – T cell responses: Cytokinesis and Cooperation
32. Tabitha was concerned when she returned from her trip to China that she had contracted Coronavirus. *Gasp.* Which of the following would be elevated if Tabitha was dying of this most recent plague?
-
IL4
-
IL17
-
IL12
-
TGF-β
-
TGF-α
33. Eugine was recently found to have a mutation in the FoxP3 gene. Which of the following would be affected?
-
Th1 response
-
Th2 response
-
Treg response
-
Th17 response
-
Macrophage response
34. Which of the following is not associated with defective Th17 immunity?
-
APECED
-
HyperIgM syndrome
-
AIRE deficiency
-
Autosomal recessive HyperIgE syndrome
-
Autosomal dominant HyperIgE syndrome
35. A new cancer drug just hit the market that affects the promotion of tumor immunity. Which of the following is a potential mechanism of action for the new drug?
-
INFγ antagonist
-
INFγ agonist
-
TGFβ antagonist
-
TGFβ agonist
36. Which of the following tells the order of events that occur in order to mount an effective response from the adaptive immune response?
-
Activation of follicular T cells, activation of T helper cell, B cell proliferation, class switching
-
B cell proliferation, class switching, activation of T helper cell, activation of follicular T cells.
-
B cell proliferation, Activation of T helper cell, activation of follicular T cells, class switching
-
Activation of T helper cell, activation of follicular T cells, B cell proliferation, class switching
-
Class switching, activation of follicular T cells, activation of T helper cells, activation of B cell proliferation.
Session 76 – B Cell Development
37. A blood sample from your patient displays a plethora of immature B cells in their periphery. The B cell surface markers present are those post B cell V(D)J recombination completion. What cell surface markers are present/absent in your patient?
-
CD19+, CD20+, Heavy𝞵+, ƛ5-
-
CD19+, CD20-, Heavy𝞵+, ƛ5+
-
CD19+, CD20+, Heavy𝞵+, ƛ5+
-
CD19+, CD20+, Heavy𝞵-, ƛ5+
-
CD19-, CD20+, Heavy𝞵+, ƛ5+

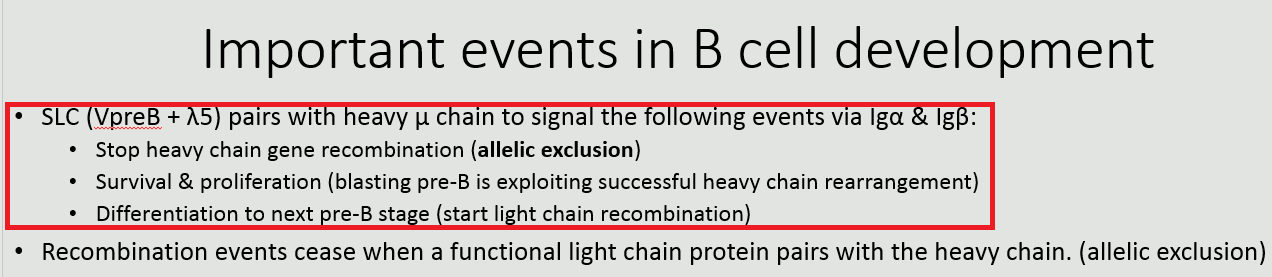
38. A blood sample from your patient displays a plethora of immature B cells in their periphery. The B cell surface markers present are those post B cell V(D)J recombination completion. In a normal individual, what event is LEAST likely to occur next when developing their TCR?
-
Allelic exclusion at the Heavy 𝞵 chain locus
-
Proliferation (blasting pre-B)
-
VpreB and ƛ5 pairing with Heavy 𝞵 chain
-
V(D)J recombination of the light chain
-
Intracellular signaling via Ig𝝰 and Ig𝛃
39. A serum sample study displays the inability of your patient’s B cells to complete their final stage of maturity in the periphery. What cell surface markers are present on these immature naive B cells?
-
CD19+, CD20+, IgM-, IgD+
-
CD19+, CD20+, IgM+, IgD+
-
CD19-, CD20+, IgM+, IgD+
-
CD19+, CD20+, IgM+, IgD-
-
CD19+, CD20+, IgM-, IgD-

40. Your 9 month old patient has developed recurrent respiratory infections. Sputum cultures are positive for Streptococcus pneumoniae and Haemophilus influenzae. Most recently they were admitted to the E/R due to severe diarrheal dehydration. Fecal samples tested positive for Salmonella species. Flow cytometry was performed for the following immuno-markers and the following results were obtained. Skin was found to be non-eczematous and platelet counts were of normal range. What condition or deficiency best explains the symptomatology and lab results of your infantile patient?


-
ADA deficiency: X-linked SCID
-
RAG1/2 deficiency
-
BTK deficiency: Agammaglobulinemia
-
DiGeorge Syndrome
-
Wiskott-Aldrich Syndrome

41. Your 9 month old patient has developed recurrent respiratory infections. Sputum cultures are positive for Streptococcus pneumoniae and Haemophilus influenzae. Most recently they were admitted to the E/R due to severe diarrheal dehydration. Fecal samples tested positive for Salmonella species. Skin was found to be non-eczematous and platelet counts were of normal range. Respiratory and diarrheal infections did not occur until after 6 months of age for your patient. What is the reasoning behind the delayed onset of these severe, recurrent infections taking hold?
-
Expression of infantile CD19 and IgD confer initial protection against pathogens during the first 6 months of life.
-
IgE from the mother’s breast milk provided passive immunity against mucosal surface infections.
-
Transplacental IgA conferred passive immunity against exogenous pathogens.
-
Increased NK and T lymphocyte production allowed for Th1 and Th17 responses to exert cytotoxic effects against invading pathogens.
-
Passive immunization via maternal transplacental IgG.

Session 77 – B Cell Responses and Immunodeficiency
42. What process/es occur in the dark zone of the germinal center in the follicles of peripheral lymphoid organs?
-
Selection
-
Selection and Antigen Capture
-
Somatic Hypermutation
-
Class Switch Recombination
-
Somatic Hypermutation and Class Switch Recombination
43. Which two cells are involved in “linked recognition”?
-
B and T cells
-
B and Th cells
-
B and Treg cells
-
B and Dendritic cells
-
T and Dendritic cells
44. What processes are occuring at B in the following figure?

-
Scanning and Proliferation
-
Scanning and Class Switch Recombination
-
Class Switch Recombination and Somatic Hypermutation
-
Scanning and Antigen Capture
-
Antigen Capture and Proliferation
45. Why would it be beneficial to give a polysaccharide conjugated vaccine over a purified conjugated vaccine?
-
High affinity IgG against the polysaccharide with a second exposure
-
Low affinity IgM against the polysaccharide with a second exposure
-
Increased affinity IgE in a type I hypersensitivity reaction
-
Low affinity IgA because polysaccharide disrupts the J-chain dimerization
-
The purified conjugated vaccine gets taken up by immune complexes, and polysaccharide conjugated vaccines activate complement to prevent immune complex buildup
46. Which immunoglobulin would be increased with a defect in T cell immunity?
-
IgM
-
IgG
-
IgE
-
IgA
-
IgD
Session 78 – Regulation of Immune Response
47. Which of the following is true regarding immune-privileged sites?
-
Costimulatory molecules are increased as a compensatory mechanism
-
Fas is expressed by some immune-privileged sites to induce apoptosis of T-cells which enter these cells
-
IgG levels in the cerebrospinal fluid are greatly reduced
-
Include the brain, spinal cord, eyes, parts of reproductive system, and heart
-
Immune privilege functions independently of homeostatic status
48. What is the function of a Fas-FasL synapse?
-
The cell expressing Fas induces apoptosis of the cell expressing FasL
-
The cell expressing Fas induces proliferation of the cell expressing FasL
-
The cell expressing FasL induces apoptosis of the cell expressing Fas
-
The cell expressing FasL induces proliferation of the cell expressing Fas
-
The cell expressing FasL with begin expressing Fas when stimulated
49. Which of the following is true regarding regulatory T-cells (Tregs)?
-
A single Treg can only act on a single T-cell, requiring a large amount of Tregs to be produced for a significant effect.
-
The transcription factor FOXP3 inhibits the production of Tregs
-
Tregs are derived of CD8+ cytotoxic T-cells
-
Tregs are produced in the periphery in response to increased recognition of self antigen or overabundant stimulation by specific non-self antigens
-
Tregs inhibit neighboring CD4 helper T-cells via secretion of IL-10 and TGF-β
50. For a patient with overactive production of CTLA-4 receptors on the surface of their T-cells, which of the following is true?
-
The CTLA-4 receptors will outcompete the CD86/CD80 receptors to bind to the CD28 surface markers.
-
The immune system will be hyperactive.
-
The patient will have an increased likelihood of developing autoimmune diseases
-
The production of primary signals will be decreased.
-
The T-cells must be activated to express CTLA-4
51. Treatment with a PD-1 blockade can result in which of the following?
-
Decreased activity of cancers, particularly melanoma
-
Decreased autoimmune diseases of epithelia
-
Decreased CTL immunity
-
Decreased production of second signals
-
Similar activity to that of CTLA-4
Session 79 – Immune Response to Infection
52. Which of the following is the first serological marker following a Hepatitis B Viral (HBV) infection?
-
HBsAg
-
Anti-HBe
-
Anti-HBc IgM
-
Anti-HBc IgG
-
Anti-HBsAg
53. An elevation in which of the following would indicate an acute HBV infection?
-
HBsAg
-
Anti-HBe
-
Anti-HBc IgM
-
Anti-HBc IgG
-
Anti-HBsAg
54. Detection of which of the following would indicate recovery and immunity from an HBV infection?
-
HBsAg
-
Anti-HBe
-
Anti-HBc IgM
-
Anti-HBc IgG
-
Anti-HBsAg
55. Which of the following is the major protective antibody that develops following administration of the hepatitis B vaccine?
-
HBsAg
-
HBeAg
-
Anti-HBc IgM
-
Anti-HBc IgG
-
Anti-HBsAg
56. An elevation in which of the following would indicate that the individual is currently infectious and the virus is replicating?
-
HBsAg
-
HBeAg
-
Anti-HBc IgM
-
Anti-HBc IgG
-
Anti-HBsAg
57. Which of the following would you expect to be elevated in a patient with a chronic hepatitis B infection?
-
HBV DNA
-
Anti-HBc IgM
-
Anti-HBe
-
Anti-HBsAg
-
Some other wrong answer
Session 80 – Hypersensitivities
58. Which of the following stimulates IgE class-switch?
-
IL-2
-
IL-3
-
IL-4
-
IL-5
-
IL-6
59. Which type of hypersensitivity is caused by the complement activating antibodies mechanism?
-
Type I
-
Type II
-
Type III
-
Type IV
-
Type V
60. A patient presents with a severe allergic reaction, which of the following is indicative of the late phase response?
-
Vasodilation
-
Heparin
-
Vascular leakage
-
Eosinophils infiltrating tissues
-
Eosinophil Chemotactic factor A
61. A patient presents with a non-cytotoxic antibody binding type 2 HS, which of the following is in your differential?
-
Incompatible blood transfusion
-
Myasthenia gravis
-
HDN
-
Hemolytic Anemia
-
Goodpasture’s Disease
62. Which of the following is characteristic to causing Hemolytic Disease of the Newborn?
-
Rh- mom, Rh- fetus
-
Rh+ mom, Rh-fetus
-
Rh+ mom, Rh+ fetus
-
Rh- mom, Rh+ fetus
-
Fetus producing anti-Rh IgG
63. A patient presents during an Arthus Reaction, which of the following is not characteristic of this hypersensitivity ?
-
Mast-Cell degranulation
-
Anaphylotoxins
-
PMN chemotaxis
-
Stimulates release of lytic enzymes from PMNs
-
Th1 helper cells/ macrophagic response
64. A patient present with a Poison Oak hypersensitive reaction, which of the following is characteristic of this reaction?
-
Sensitization on the First encounter
-
Th1 pro-cellular immunity on the First encounter
-
Complement activation on the First encounter
-
Circulating Immune complex activation on First Encounter
-
Degranulation and Eosinophil rxn on First encounter
65. Which harmful characteristic is also related to the hypersensitivity that is protective against extracellular viral particles?
-
Systemic anaphylaxis
-
Localized anaphylaxis
-
Hemolytic anemia
-
Serum sickness
-
Rheumatoid arthritis
66. Which autoimmune disease has anti-AchR antibodies found in circulation along with signs of ptosis?
-
Type 1 Diabetes Mellitus
-
Myasthenia Gravis
-
Graves’ Disease
-
Lupus Nephritis
-
Hemolytic Anemia
67. Anti-Type 4 collagen IgG antibodies along with fatigue, nausea, and respiratory distress are signs of which autoimmune disease?
-
Type 1 Diabetes Mellitus
-
Myasthenia Gravis
-
Lupus Nephritis
-
Goodpasture Syndrome
-
Graves’ Disease
68. Which autoimmune disease presents as a Type 2 Hypersensitivity with low TSH and high T4 levels?
-
Myasthenia Gravis
-
Lupus Nephritis
-
Graves’ Disease
-
Type 1 Diabetes Mellitus
-
Addison’s Disease
69. Which autoimmune disease is positive for HLA-B27?
-
Addison’s Disease
-
Crohn’s Disease
-
Celiac Disease
-
Psoriasis
-
Ankylosing spondylitis
70. Elevated MSH and mucosal hyperpigmentation are characteristics of what autoimmune disease?
-
Addison’s Disease
-
Crohn’s Disease
-
Celiac Disease
-
Psoriasis
-
Ankylosing spondylitis
71. Which of the following would be considered a systemic autoimmune disease?
-
MS
-
Rheumatoid Arthritis
-
Addison’s Disease
-
Psoriasis
-
Crohn’s Disease
72. Administration of which of the following would be consistent with treating symptoms versus global immunosuppression?
-
TNF-alpha inhibition
-
TNF-beta inhibition
-
Corticosteroids
-
Non-steroidal anti-inflammatories
-
Prednisone
Session 82 – Cellular Adaptation
73. Barret’s esophagus is an adaptive response in patients with GERD where the squamous cells of the esophagus are replaced by glandular cells. This is an example of…
-
Hypertrophy
-
Atrophy
-
Hyperplasia
-
Metaplasia
-
Hypermetaplasia
74. P53 is able to start a pro-apoptotic cascade after being phosphorylated by either ATM or…..
-
BCL2
-
Chk1
-
MDM2
-
AKT
-
BAX
75. Amyloidosis occurs when proteins are deposited in the extracellular space of various tissues or organs. If a patient is presenting with non-Ig protein deposition, then what type of amyloidosis do they most likely have?
-
Primary Amyloidosis
-
Secondary Amyloidosis
-
Beta-Amyloidosis
-
Transthyeretin (TTR) Amyloidosis
-
Localized Amyloidosis
76. Which of these characteristics would be indicative of an irreversible injury?
-
Membrane blebbing
-
Organelle swelling
-
Slowly recovering mitochondrial dysfunction
-
Cellular content leaking
-
Severe membrane swelling
77. Pathologic hypertrophy signalling cascades results in which three transcription factors?
-
IGF-1, AKT, JAK-STAT
-
IGF-1, MEF-2, AKT
-
MEF-2, JAK-STAT, AKT
-
NFAT, MEF-2, JAK-STAT
-
NFAT, MEF-2, IGF-1
Session 86 – Mechanisms of Inflammation
78. Which of the following correctly matches the Leukocyte adhesion deficiency with the symptom?
-
Delayed umbilical cord detachment: LAD II
-
Bombay blood type: LAD III
-
Most severe infections: LAD II
-
Absence of pus at infection site: LAD I
-
Less severe infections: LAD I
79. Joy gave birth to a beautiful baby boy. Unfortunately her three-month-old he has been chronically sick in his first few months on earth and was recently diagnosed with Chronic granulomatous disease. Which of the following is he least likely to have had in the last three months?
-
Streptococcus
-
Staphylococcus aureus
-
Listeria
-
Candida
-
Aspergillus
80. Which of the following is consistent with chronic inflammation?
-
Tissue damage followed by fibrosis and angiogenesis
-
Presence of mostly neutrophils
-
Acute exposure to foreign bodies or allergens lead to it
-
Decreased angiogenesis
-
Presence of macrophages, lymphocytes or plasma cells
81. Chronic inflammation is associated with which type of hypersensitivity?
-
Autoimmune diseases
-
Type I
-
Type II
-
Type III
-
Type IV
82. Which of the following is not consistent with granulomas?
-
Compact aggregate of activated macrophages
-
Central necrosis surrounded by lymphocytes caused by Th1 (usually) responses
-
Treatment with anti-TNF is the preferred treatment for granuloma
-
Can be caused by bartonella, coccidioides, or chlamydia
-
Can be caused by listeria, mycobacterium, or blastomyces
83. Which of the following correctly matches what occurs with each type of pathological calcification?
-
Dystrophic calcification: increased serum Ca
-
Dystrophic calcification: occurs in cancer
-
Metastatic calcification: occurs in hypoparathyroidism
-
Metastatic calcification: seen in patients with DiGeorge syndromes
-
Metastatic calcification: seen preferentially in the stomach
Session 87 – Tissue Renewal, Regeneration, and Repair
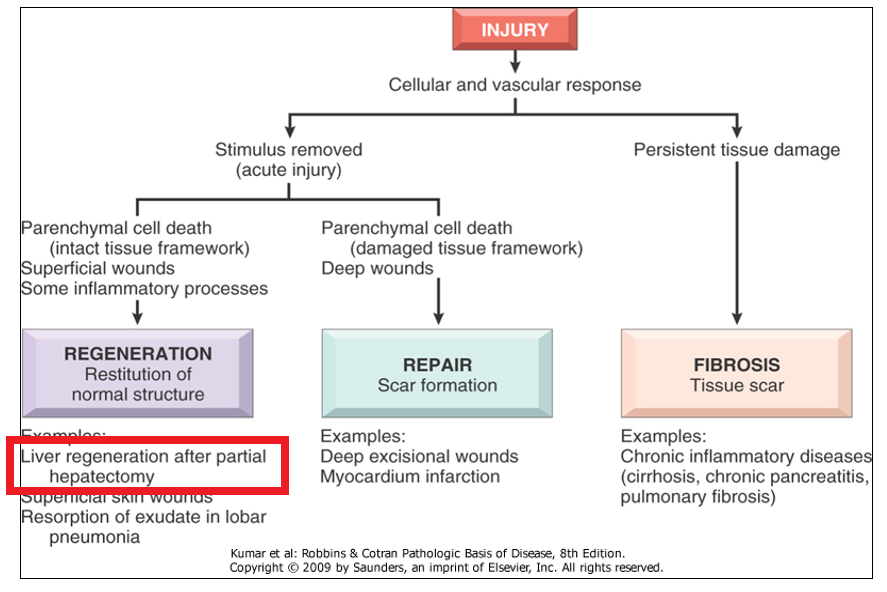
84. Which of the following situations/conditions would allow for the regeneration and restitution of normal tissue structure following tissue injury?
-
Pulmonary Fibrosis
-
Myocardial infarction
-
Hepatic cirrhosis
-
Partial hepatectomy
-
Chronic pancreatitis
85. Your adolescent patient presents with general weakness; pallor and SOB; swollen cheeks and jaw; and diffuse neoplasms across his skin. The following CBC with differential was provided and confirmed by your pathologist coworker you went to ARCOM with. Genetic testing reveals excessive activation of proliferative signaling pathways governing his labile tissues only. Which organ system(s) are you not concerned about in developing excessive growth and proliferation?

-
Cuboidal epithelial cells of the parotid gland
-
Hematopoietic cells of the bone marrow
-
CNS and cardiomyocytes
-
Intralobular ducts of the pancreas
-
Squamous epithelia of the conjunctiva
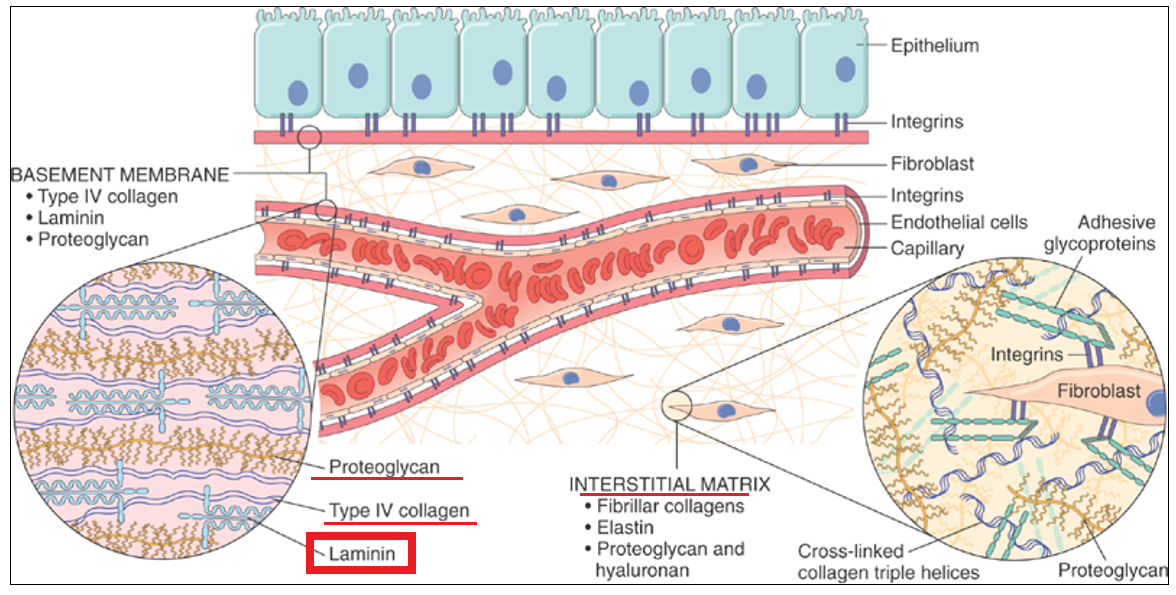
86. Your patient presents with extensive, large fluid-filled blisters across his arms, legs, and fold areas of their skin. Before jumping the gun on your diagnosis, you take a biopsy and send it to pathology. Pathologic microscopic analysis reveals intact connections between the surface epithelium and basement membrane, but there is a plethora of fragmented debris from a key connective tissue component that connects the Type IV Collagen to the Proteoglycans in the Interstitial Matrix. Which component of the IM is being pathologically degraded?
-
Hyaluronan
-
Laminin
-
Elastin
-
Integrins
-
Fibroblasts
87. The year is 1612, and you are coupling your recent medical knowledge with your yearn to explore the new world; working as the only medical physician aboard a ship as you sail across the Atlantic Ocean. Several of your crew have been experiencing easy bruising and extreme fatigue. An oral inspection reveals bleeding gingival tissues. The cook shares with you that none of the oranges brought aboard have been eaten, and that the rum’s all gone. The formation of what AA derivative that requires oranges as a cofactor is essential for maintaining the triple helix structure of collagen fibrils, and whose deficit is leading to the symptoms seen by the crew?
-
Heparin sulfate
-
Hydroxyproline
-
Hyaluronic acid
-
Keratan sulfate
-
Chondroitin sulfate

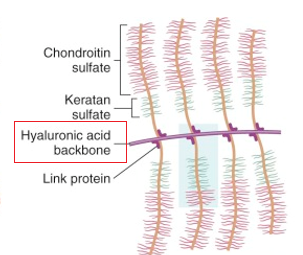
88. A new dietary fad that has been sweeping the nation is adding trace micro-concentrations of metalloids to water and sports drinks. Since this craze you have noticed a trend of complaints concerning joint and tissue problems in individuals who have adopted this new trend. A tissue biopsy and microanalysis from your patient reveals the deposition of Arsenic on the backbone component of the proteoglycan matrix. Where on the proteoglycan has this metalloid accumulated?
-
Elastin
-
Keratan sulfate
-
Chondroitin sulfate
-
Hyaluronic acid
-
Syndecan
89. Which cell is responsible for the production of collagen fibrils that constitute the extracellular matrix?
-
Fibroblasts
-
Mesenchymal cells
-
Vascular Endothelial cells
-
Laminar cells of the basement membrane
-
Keratinocytes
90. Biopsy results from an uncertain neoplasm that you took reveal an overabundance of endothelial cells, suggesting abnormal angiogenesis to support this abnormal tissue growth. Which growth factor is responsible for the enhanced proliferation of endothelial cells along with increased vascular permeability?
-
TGF-β
-
FGF
-
VEGF
-
PDGF
-
EGF

91. Which of the following statements about neoplasms is true?
-
Adenocarcinomas arise in glandular epithelial cells that secrete substances
-
Carcinomas are derived from connective tissues or supportive tissues
-
Leukemias are tumors of B-cells and T-cells
-
Lymphomas have clear margins making them amenable to removal
-
Sarcomas are benign
92. Which of the following key characteristics of neoplasms is true?
-
Anaplasia is commonly seen in malignant tumors
-
Benign tumors are poorly differentiated
-
Malignant tumors are well-demarcated due to invasion of surrounding tissues
-
Metastasis is more likely with small, differentiated tumors
-
Mitotic figures are commonly seen in benign tumors
93. In regards to carcinogenesis/mutagenesis, which of the following scenarios would result in the formation of a tumor? CO = Croton oil, a promoter; PH = polycyclic hydrocarbon, an initiator.
-
Application of CO followed by PH to test cells
-
Application of CO to test cells
-
Application of PH followed by CO to test cells
-
Application of PH to test cells
-
None of the above would cause formation of a tumor
94. Which of the following lists the correct mutation to the respective gene/protein as seen in the common accumulation of mutations in the progression of cancer?
-
DNA hypermethylation
-
Gain of p53
-
Loss of kRAS (RAS/MAPK pathway)
-
Loss of PARP
-
Overexpression of APC
95. Which of the following cancer causing microbes is an oncogenic RNA virus?
-
Epstein-Barr virus
-
H. pylori
-
Hepatitis B
-
Human papillomavirus (HPV)
-
Human T-cell leukemia virus type 1 (HTLV-1)
96. For the “sustained proliferative signalling” pillar in the hallmarks of cancer ideology, which of the following is true?
-
Gain of function mutations increase
-
Reduced expression of ligand receptors on the cell surface
-
Shift from autocrine signalling to paracrine signalling
-
Shift from ligand-independent firing of receptors to ligand-dependent firing of receptors
-
Shift of oncogenes to proto-oncogenes
97. For the “evasion of growth/tumor suppression” pillar in the hallmarks of cancer ideology, which of the following is true?
-
Growth inhibitors act on RB through hyperphosphorylation, which inactivates it and reduces its transcription effect
-
Involves gain of function mutations
-
Key tumor suppressor genes include p53, RB, APC, BRCA1/2, and VHL
-
Most tumors are genetically dominant
-
Sporadic retinoblastoma forms from only a single mutation to the RB locus in retinal cells, whereas familial retinoblastoma forms from two mutations to the RB locus in retinal cells
98. For the “replicative immortality” pillar in the hallmarks of cancer ideology, which of the following is true?
-
Breakage-fusion-breakage cycles lead to abnormal karyotypes, particularly translocations and aneuploidy
-
Fusion of unprotected chromatids can only occur between homologous chromosomes due to length restrictions
-
In cancerous cells, reduced expression of telomerase leads to increased telomere which prevents their senescent apoptosis
-
Normal cell chromosomes progressively gain longer telomeres with repeated replication which leads to apoptosis
-
Progressive loss of telomeres is directly proportional to increased expression of the p53 gene
99. For the “resisting cell death” pillar in the hallmarks of cancer ideology, which of the following leads to decreased likelihood of apoptosis as seen in cancerous cells?
-
Increased expression of BIM or PUMA (BH3-only proteins)
-
Increased expression of SMAC/DIABLO
-
Loss of BAK/BAX
-
Loss of BCL2 proteins
-
Overactivation of Caspase 3
100. For the “metabolic alterations” emerging hallmark of cancer, which of the following is true for the Warburg effect?
-
Growth factors stimulate receptor tyrosine kinases to activate increased glucose transporters in cancerous cells
-
The cancerous cell increases lipid and amino acid catabolism
-
The cancerous cell increases mitochondrial oxidative phosphorylation to increase glycolytic intermediates for use in cellular growth
-
The major depletion of energy in quiescent cells is synthesis of nucleotides, amino acids (proteins), and lipids
-
Quiescent cells open glutamine channels to use glutamine for a primary metabolic fuel
Session 90 – Renal System Histology I
101. Which renal system function is the most important in maintaining blood pH values?
-
Regulation of Balance
-
Excretion
-
Secretion
-
Conversion
-
Gluconeogenesis
102. Which renal system function is the most important in the activation and concentration of aldosterone?
-
Regulation of Balance
-
Excretion
-
Secretion
-
Conversion
-
Gluconeogenesis
103. Which renal system function is the most important in drug/medication clearance?
-
Regulation of Balance
-
Excretion
-
Secretion
-
Conversion
-
Gluconeogenesis
104. Which renal system function is the most important in maintaining calcium serum levels?
-
Regulation of Balance
-
Excretion
-
Secretion
-
Conversion
-
Gluconeogenesis
105. An occlusion in an interlobular artery (aka cortical radiate artery) would prevent blood from entering into which of the following types of arteries?
-
Renal Artery
-
Peritubular capillaries
-
Interlobar artery
-
Segmental Artery
-
Arcuate Artery
106. Which of the following is true regarding a difference between cortical and juxtamedullary nephrons?
-
There are less cortical nephrons than juxtamedullary
-
Individual juxtamedullary nephrons receive more blood flow than individual cortical nephrons
-
Juxtamedullary nephrons are longer and their loop of henle dives deep into the medulla
-
Juxtamedullary nephrons are located entirely in the medulla while cortical are located entirely in the cortex
-
Juxtamedullary nephrons are only concerned with concentration and thus do not have a proximal convoluted tubule (PCT) or distal convoluted tubule (DCT)
107. Which type of epithelium is located in the proximal convoluted tubule (PCT)?
-
Simple squamous
-
Simple cuboidal
-
Simple columnar
-
Stratified squamous
-
Pseudostratified columnar
108. Which type of cells make up the visceral layer of the renal corpuscle?
-
Simple squamous
-
Endothelium
-
Simple cuboidal
-
Mesothelium
-
Podocytes
109. Which of the following filtration barriers is the most selective in what it allows to pass?
-
Fenestrated capillaries
-
Sinusoidal capillaries
-
Glomerular basement membrane
-
Podocyte basement membrane
-
Podocyte filtration slits
110. Which of the following molecules would not be able to pass through the filtration barrier in a healthy glomerulus?
-
Water
-
Glucose
-
Sodium
-
Albumin
-
Hydrogen ions

111. In the image above, what is the structure being pointed at?
-
Renal Corpuscle
-
Proximal convoluted tubule
-
Loop of Henle
-
Distal convoluted tubule
-
Collecting Duct
Session 91 – Renal System Histology II

112. According to the image above, which of the following begins simple cuboidal before transitioning to columnar epithelial cells?
-
A
-
B
-
C
-
D
-
E
113. Over half of the water and electrolytes and all of the organic nutrients are reabsorbed in this section?
-
Glomerulus
-
PCT
-
Loop of Henle
-
DCT
-
Collecting Duct
114. What type of epithelium is found in the thick ascending limb of the loop of henle?
-
Simple Squamous
-
Pseudostratified Squamous
-
Simple Columnar
-
Simple Cuboidal
-
Stratified Columnar
115. This is the layer that is modified creating the juxtaglomerular granular cells?
-
Tunica interna
-
Tunica media
-
Tunica externa
-
Tunica prima
-
Tunica secundum
116. Which Nephron structure contains aquaporins?
-
Collecting Duct
-
DCT
-
Loop of Henle
-
PCT
-
Juxtaglomerulus Apparatus
117. Which of the following is NOT characteristic of umbrella cells?
-
Large and bulbous shape
-
Elliptical shape
-
Protect the cells beneath from hypertonic urine
-
Trinucleated
-
Highly differentiated
118. Which of the following is NOT a histological layer of the bladder?
-
Urothelium
-
Submucosa
-
Muscular layer
-
Adventitia
-
Lamina Densa
119. Which of the following is not a sign or symptom of Glomerulonephritis?
-
Hematuria
-
Hypertension
-
Proteinuria
-
Cystitis
-
Edema
Session 92 – Renal System Development
120. Which of the following list structures seen during the development of the kidneys in the correct chronological order of which they appear?
-
Pronephros, mesonephros, metanephros, urogenital ridge, nephrogenic cord
-
Pronephros, urogenital ridge, mesonephros, nephrogenic cord, metanephros
-
Urogenital ridge, nephrogenic cord, pronephros, mesonephros, metanephros
-
Urogenital ridge, pronephros, mesonephros, metanephros, nephrogenic cord
-
Urogenital ridge, pronephros, mesonephros, nephrogenic cord, metanephros
121. Which of the following embryological structures predominantly persist past fetal development as functional structures in a delivered child?
-
Allantois
-
Cloaca
-
Mesonephros
-
Metanephros
-
Pronephros
122. Which of the following correctly describes the process of the relative ascent of the kidneys?
-
It begins in the 6th week (with the mesonephros) and ends around the 9th week
-
The kidneys each rotate 90 degrees ventrally
-
The process joins each suprarenal gland and its associated kidney closer together until juxtaposition
-
The same arteries supply the kidneys throughout the whole process, preventing supernumerary arteries
-
Relative movement of the kidneys is caused by the cranial part of the embryo growing away from the kidneys
123. The allantois is obliterated into which of the following structures in an adult?
-
Ligamentum venosum
-
Ligamentum teres
-
Medial umbilical ligament
-
Median umbilical ligament
-
Lateral umbilical ligament
124. A three week old female is brought into the pediatric clinic for a urinary tract infection. In the physical exam of the pelvis you note a single orifice, presumably the anus but no urethra or vagina. During your HPI, the parents tell you that she was a home birth and that her diapers show that she still passes both urine and feces. Which embryological structure failed to form properly between the fifth and twelfth week of development?
-
Cloaca
-
Mesonephric duct
-
Urachus
-
Ureteric bud
-
Urorectal septum
125. Which of the following statements about the development of the metanephros is true?
-
The connecting tubule is formed from the metanephrogenic bud
-
The metanephrogenic blastema forms the collecting system section of the kidney
-
The S-shaped renal tubules differentiate to form the metanephric vesicles
-
The ureteric bud forms the nephron section of the kidney
-
The urethra is formed from the ureteric bud
Session 93 – Glomerular Filtration and Renal Blood Flow I
126. Which cells are responsible for the paracrine signaling of renin?
-
Intraglomerular
-
Granule Cells
-
Podocytes
-
Pedicels
-
Myocytes
127. Glomerular filtration of proteins would occur at which cell layer?
-
Glomerular capillary wall
-
Fenestrated endothelial cells
-
Basement membrane
-
Bowman’s capsule
-
Filtration Slits
128. Which of the following could cause a decrease in the GFR?
-
Defective nephrin protein
-
Lifting of podocytes
-
Proliferation of podocytes
-
Thinning of podocytes
-
Increased filtration slit distance
129. Calculate the COP with a GFR of 5mmHg, PGC of 45, and PBS of 25mmHg?
-
5
-
10
-
15
-
20
-
25
130. Which will cause a decrease in the Net Filtration Pressure?
-
Dilation of afferent arteriole
-
Constriction of afferent arteriole
-
Constriction of efferent arteriole
-
Increased PGC
-
Decreased PBS
Session 94 – Glomerular Filtration and Renal Blood Flow II
131. What is a normal GFR (mL/min) using Inulin clearance as an indirect measurement?
-
85
-
100
-
115
-
130
-
145
132. An elderly patient is in your care and you are tasked with calculating his GFR with the given values: PInulin = 3mg/mL, UInulin = 260mg/mL, V = 1.5mL/min. GFR = ….
-
125mL/min
-
130mL/min
-
140mL/min
-
160mL/min
-
100mL/min
133. The macula densa is activated by which stimuli in the tubuloglomerular feedback loop?
-
Increased Adenosine/ADP/AMP
-
Low GFR
-
High NaCl
-
Vasoconstriction of the AA
-
Activation of the extraglomerular mesangial cells
134. Low doses of angiotensin II will cause what effect?
-
↑RBF
-
↑ Resistance in AA
-
↑GFR
-
↓FF
-
↓Resistance in AA
135. Why is inulin often used as an indirect measurement of GFR?
-
Plasma Inulin and Secreted Inulin are both overestimated by 20%
-
Inulin is secreted, but not absorbed
-
Inulin is absorbed, but not secreted
-
Inulin is secreted and absorbed
-
Inulin is neither secreted nor absorbed
Session 95 – Glomerular Filtration and Renal Blood Flow III
136. Which of the following correctly explains how renin is released into the bloodstream?
-
The macula densa senses low salt causing renin to be released from granular cells into the efferent arteriole.
-
The macula densa senses low salt causing renin to be released from granular cells into the afferent arteriole.
-
The macula densa senses high salt causing renin to be released from granular cells into the efferent arteriole.
-
The macula densa senses high salt causing renin to be released from granular cells into the afferent arteriole.
-
The macula densa senses low salt causing renin to be released from the macula densa into the efferent arteriole.
137. Which of the following is not a direct effect of Angiotensin II?
-
Vasoconstriction
-
Release of aldosterone
-
Release of antidiuretic hormone
-
Sodium reabsorption
-
Water reabsorption
138. Which of the following is true of Angiotensin II?
-
Relaxes arterial smooth muscle causing a decrease in mean arterial pressure
-
Triggers the kidney to release aldosterone to increase Na reabsorption
-
Constricts the afferent arteriole but not the efferent arteriole
-
Causes an increase in Kf which results in an increase in GFR
-
It acts directly in the proximal and distal renal tubules
139. Which of the following is false regarding Atrial Natriuretic Peptide?
-
It is secreted by the atria in response to sodium retention
-
It inhibits sodium reabsorption in the distal part of the nephron
-
It opposes aldosterone
-
It inhibits renin secretion while dilating the efferent arterial and constricting the afferent arteriole
-
It causes an increase in both renal plasma flow and glomerular filtration rate
140. Your attending tells you that you can be first assist on a ureteroscopy if you can correctly answer the following question: In which of the following would you first see infarctions in the kidney? Thinking back to what you learned from your physiology and histology lectures, you respond:
-
Glomerulus
-
Proximal convoluted tubule
-
Loop of Henle
-
Distal convoluted tubule
-
Afferent arteriole
-
Efferent arteriole
141. While on your ER rotation, a 55 year old obese caucasion male comes in with SOB, edema in his lower extremities, nausea, fatigue and extreme weakness. While taking his history you find out that he is a construction manager who is under a lot of stress to complete his most recent project. He has two kids and is in a monogamous relationship with his wife of 30 years. He has a very unhealthy diet eating fast food at least once a day and does not exercise. He has been a pack a day smoker for 20 years. He drinks 1-2 beers per night. He is on lisinopril, hydrochlorothiazide, bupropion, simvastatin, sildenafil, warfarin, a multivitamin and has been taking Ibuprofen for lower back pain. He is allergic to penicillin, cats, and shellfish. Which of the following is the most likely differential diagnosis?
-
Acute renal failure
-
Liver failure
-
COPD
-
Somatic dysfunction of the lower back
-
Congestive Heart failure
142. The [plasma] of a substance at which the substance will start showing in the urine is called the what?
-
Transport Maximum
-
Splay
-
Renal Threshold
-
Filtered Load
-
Renal Clearance

143. Which intracellular condition would deter the uptake of glucose and amino acids in the PCT?
-
Low intracellular [Na+]
-
High extracellular [Na+]
-
High intracellular [K+]
-
High intracellular [Na+]
-
Low extracellular [K+]
144. Which of the following will have approximately the same concentration at both the end of the PCT and in its respective peritubular capillary region?
-
Inulin
-
Glucose
-
Sodium
-
HCO3–
-
Chloride

145. Which of the following will have a fractional delivery equal to “1” at the end of the PCT?
-
Inulin
-
Potassium
-
HCO3–
-
PAH
-
Urea

146. Which of the following characteristic(s) of a substance would make it best suited to determine the Renal Plasma Flow?
-
Something that is filtered only: not reabsorbed or secreted in the PCT.
-
Something that is filtered and reabsorbed along the PCT.
-
Something that is filtered and secreted along the PCT.
-
Something that equals its own [plasma] along the length of the PCT.
-
Something that is reabsorbed and secreted at the same rate along the PCT.
Session 97 – Tubular Reabsorption and Secretion II
147. What is the main driving force in the Proximal Convoluted Tubule?
-
NHE3 channels
-
ROMK channels
-
Na+/K+ ATPase
-
SGLT2
-
MRP ATPase
148. How does Cl- get reabsorbed in the Proximal Convoluted Tubule?
-
Active Transport
-
Symport
-
Passive Transport
-
Antiport
-
Osmosis
149. Regarding its use in the nephron, administration of a carbonic anhydrase inhibitor would cause which of the following?
-
Metabolic acidosis
-
Hypermagnesemia
-
Hyperkalemia
-
Metabolic alkalosis
-
Hypokalemia
150. Back in WWI the US was running out of penicillin to give to soldiers, so they had to come up with a better way to conserve its supply. They decided to give them penicillin, then flush them full of a bunch of other drugs as well. Why did this work?
-
The other drugs were able to treat the soldiers disease by themselves.
-
The MRP ATPase had more of a supply of ATP provided by the other drugs.
-
The electrochemical gradient increased because of the rush of positive charges.
-
Organic anion transporters are competitive and the penicillin would be able to stay in the soldiers for a longer period of time.
-
More drugs less problems.
151. Administering ANP would have which effect on the PCT?
-
Decreased filtrate concentration of NH4+
-
Increased filtrate concentration of K+
-
Increased driving force for ion movement in the PCT
-
Increased blood concentration of Cl- through active transport
-
Increased activation of ROMK channels
152. Inulin clearance by your patient was equal to 125 mg/mL. Plasma concentration of target solute is 10 mg/mL. Urine concentration of solute is 5 mg/mL and filled a 100mL cup in a minute. Calculate the solute reabsorption.
-
75 mg/min
-
100 mg/min
-
200 mg/min
-
600 mg/min
-
750 mg/min
Session 98 – Tubular Reabsorption and Secretion III
153. A patient presents with acute cerebral edema due to chugging 5 liters of water because they heard it would protect them from the corona virus. Which of the following medications would you administer to this patient first?
-
Losartan (Angiotensin receptor blocker)
-
Lisinopril (ACE inhibitor)
-
Metoprolol (Beta Blocker)
-
Mannitol (osmotic diuretic)
-
Lasix (loop diuretic)
154. Which of the following statements is true in regards to the nephron loop/loop of henle?
-
The descending limb is permeable to sodium
-
The descending limb permeability changes in regards to Angiotensin II
-
The thick ascending limb is a target of medications like Furosemide and Lasix
-
The thick ascending limb is permeable to water
-
The thick ascending limb is responsible for reabsorption of sodium through NCC
155. The charge differential created in the lumen forces which of the following ions to move paracellularly into the blood/interstitium?
-
Cl-
-
HCO3-
-
H+
-
Ca++
-
ATP
156. Which of the following ions can be substituted with K+ in NKCC and most other K+ transporters?
-
Na+
-
NH4+
-
HCO3-
-
Cl-
-
Mg++
157. Which of the following channels/transporters is most important to maintaining the functionality of the Na+/K+ ATPase in the thick ascending limb?
-
Basolateral rectifying K+ channel
-
Luminal rectifying K+ channel
-
ROMK
-
NKCC
-
NCC
158. Loop diuretics have been known to cause hypocalcemia with prolonged use. Which of the following types of medications could you give to counteract this side effect?
-
ACE Inhibitors
-
Angiotensin receptor blockers
-
Thiazide diuretics
-
Amiloride diuretics
-
Beta Blockers
159. Which of the following statements is true in regards to the osmolarity of the filtrate throughout the nephron?
-
The filtrate in the bowman’s capsule is hypotonic in comparison to the blood
-
The filtrate at the end of the collecting duct will always be the most hyperosmotic
-
The filtrate at the beginning of the loop of henle will be hyperosmotic in comparison to the blood
-
The filtrate at the end of the proximal convoluted tubule will be hyperosmotic in comparison to the blood
-
The filtrate at the end of the loop of henle will be hypoosmotic in comparison to the blood
160. Which of the following statements is true in regards to the distal convoluted tubule (DCT)?
-
It is the section in which most of the reabsorption along the nephron takes place
-
Chloride ions are primarily reabsorbed transcellularly
-
ENaCs are thiazide sensitive transporters in the DCT1
-
The DCT will be subject to hypertrophy after prolonged use of loop diuretics as a compensatory mechanism to the increased flow rate
-
NCCs in the DCT1 create a negatively charged lumen due to their function
161. Which of the following hormones does NOT increase the expression of NA+ channels in the DCT and thus increase the Na+ reabsorption?
-
ADH
-
ANP
-
Aldosterone
-
Angiotensin II
-
Insulin
162. A deficiency of which of the following ions will cause refractory hypokalemia due to its effects on ROMK channels?
-
Magnesium
-
Calcium
-
Sodium
-
Chloride
-
Bicarbonate
163. Which of the following hormones can bind to the same receptor as Aldosterone if not first inactivated by another enzyme?
-
Angiotensin II
-
Insulin
-
Cortisol
-
Estrogen
-
Vasopressin
164. Which of the following channels is essential to the transcellular reabsorption of magnesium in the DCT and can be affected by Thiazide diuretics?
-
TRPV5
-
TRPM6
-
NCC
-
ENac
-
NKCC
Session 99 – Tubular Reabsorption and Secretion IV
165. Which of the following is not a component of the collecting duct?
-
Principal Cells
-
Type A intercalated
-
Type B intercalated
-
Paracellular transport
-
Uncoupled water absorption
166. Which of the following increases ROMK activity?
-
Insulin
-
Catecholamines
-
ADH
-
AngII
-
Aldosterone
167. Which of the following has an inhibitory effect on ENaC in the collecting duct?
-
ANP
-
Insulin
-
ADH
-
Catecholamines
-
AngII
168. Which of the following is an effect of ADH?
-
Decrease aquaporin-2
-
Decreased NKCC2 at TAL
-
Increased ENaC at DCT2
-
Increased NCC at PCT
-
Increased ROMK at CD
169. Syndrome of inappropriate ADH secretion is not caused by or characteristic of which of the following?
-
Ectopic ADH production
-
Lack of hypothalamic osmoreceptors
-
Asthma
-
Ecstasy
-
Infection
170. Which of the following is characteristic of type A intercalated cells?
-
H+ ATPase is the driving active basolateral force
-
Pendrin echanges HCO3 with Cl-
-
Contains NDCBE on the lumenal side
-
Works with bases
-
Action Generates HCO3 by CAII
171. A patient presents with loss of NCC in the DCT and is diagnosed with which clinical condition?
-
Bartter’s syndrome
-
Gitelman’s syndrome
-
Diabetes Insipidus
-
Diabetes Mellitus
-
Liddle’s syndrome
Session 100 – Renal Homeostasis I
172. Severe overhydration will have what effect on the nephron?
-
Increased ADH
-
Increased UT receptors
-
Decreased UT receptors
-
Concentrated urine
-
Increased interstitial urea
173. Which of the following will not be activated due to an increase in ADH?
-
ENaC @ DCT2/CD
-
ROMK @ TAL
-
Na/K ATPase @ distal nephron
-
NCC @ PCT
-
UT-A1 @ CD
174. Which receptor is associated with the apical side of the collecting duct when AVP is upregulated?
-
V1 receptor
-
V2 receptor
-
Aquaporin 2
-
Aquaporin 3
-
Aquaporin 4
175. Normal osmolarity levels coupled with a decrease in ECF volume is an indicator of which problem?
-
Diarrhea
-
Alcoholism
-
Fever
-
Large NaCl loss
-
Edema
176. Overhydration of the ECF would have which of the following effects?
-
Increased ADH
-
ECF volume decreased
-
ICF volume decreased
-
ECF and ICF osmolarity increased
-
ECF and ICF volume increased
177. Increased ECF volume with increased osmolarity is associated with which of the following?
-
Increased ADH
-
Alcoholism
-
Vomiting
-
Aldosterone Deficiency
-
Edema
Session 101 – Renal Homeostasis II
178. Where in the nephron is the primary reabsorption of sodium occuring?
-
PCT
-
Thin Descending Limb
-
TAL
-
DCT
-
CD
179. Where will progesterone decrease sodium reabsorption?
-
PCT and TAL
-
PCT and DCT
-
TAL and DCT
-
TAL and CD
-
DCT and CD
180. When a patient becomes sodium depleted, how is their potassium concentration ultimately affected?
-
Increased potassium excretion
-
Decreased potassium excretion
-
Potassium excretion is unchanged
-
Increased potassium reabsorption
-
Decreased potassium secretion
181. In addition to being a vasodilator, ANP also inhibits the production of which hormone?
-
Renin
-
Oxytocin
-
Progesterone
-
ADH
-
Cortisone
182. Osmotic diuretics, such as Mannitol, decrease the Na concentration in the PCT by increasing the filtrate volume. This in turn causes Na to back flow towards the filtrate. What pathway does Na predominantly take as it tries to re-enter the PCT?
-
Na, K, ATPase
-
NHE3
-
Transcellular
-
Paracellular
-
NKCC
Session 102 – Metabolism of the Kidney/Renal Function Measure
183. Which of the following is true regarding gluconeogenesis in the kidney but not in the liver?
-
It can release glucose directly into the blood
-
It uses little to none of the glucose it makes
-
Alanine is the prefered amino acid
-
Lactate is the substrate used to make glucose
-
This process is done when insulin is low
184. Where in the kidney does gluconeogenesis occur?
-
Proximal convoluted tubule
-
Collecting duct
-
Renal cortical cells
-
Inner renal medullary cells
-
Outer renal medullary cells
185. While rotating in the ED, EMS arrives with a 54 year old male in ketoacidosis. Which of the following is the most concerning factor that could cause his body to go into a diabetic coma if left untreated/before you administer anything?
-
Decreased insulin
-
His acidotic state
-
Fruity breath
-
Increased insulin
-
His alkalotic state
186. Which of the following is false in the renal system?
-
Insulin increases glucose uptake
-
Insulin increases glycerol and lactate uptake
-
Insulin increases glucose release
-
Glucagon does not affect glucose release
-
Epinephrine increases glucose release
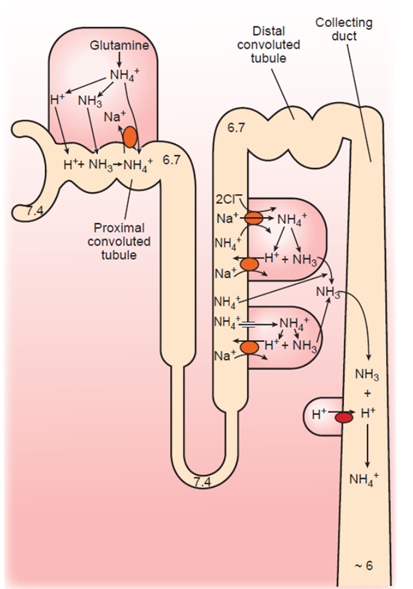
187. Which of the following is not used to move ammonia/ammonium?
-
Diffusion at PCT
-
NHE3 at PCT
-
NKCC at TAL
-
Diffusion at TAL
-
NHE4 at TAL
188. A mutation in NHE4 would cause which of the following?
-
Increased NH3 in the urine
-
Increased NH4 in the urine
-
More acidic urine
-
Increased diuresis
-
Dilute urine
Session 103 – Renal Acid Base Regulation
189. To calculate the [titratable], one would need to do which of the following?
-
Subtract the [HCO3-] from the [NH4+] in the urine.
-
Measure the mEq of [HCO3-] need to return the urine back to neutral blood pH.
-
Subtract the [H2PO4-] from the [NH4+] in the urine.
-
Measure the mEq of [OH-] needed to return the urine back to neutral blood pH.
-
Use a litmus strip to determine the urine acidity.
190. Where in the nephron would we see the highest [HPO4–]?
-
Bowman’s capsule
-
Distal PCT
-
Distal TAL
-
Distal convoluted tubules
-
Proximal end of collecting duct
191. Where in the nephron would we see the highest [H2PO4-]?
-
Proximal end of the PCT
-
End of the thin descending limb.
-
Bowman’s capsule
-
Distal end of the PCT
-
Midway region of the PCT

193. A decrease in blood pH causes which of the following?
-
Decreased NHE3 activity
-
Increase in ammonia synthesis
-
Decrease in Na+/K+ ATPase
-
Decrease in glutamine transporters
-
Increase in NH3 resorption from the filtrate

194. Which of the following conditions is most likely to lead to acute metabolic acidosis?
-
Increase in Angiotensin II
-
Increased ROMK
-
Stimulation of ENaC
-
Increased Aldosterone
-
Hyperkalemia

Session 104 – Genetic Disorders of the Renal System
195. A patient comes to the clinic complaining of trouble hearing, and when taking a family history you realize they are at risk for a Type IV collagen disorder. A Urinalysis showed albuminuria and proteinuria. Which of the following disorders matches the inheritance pattern found in this patient’s disorder?
-
Sickle Cell Anemia
-
ARPKD
-
Marfan’s Syndrome
-
Hemophilia A
-
Tay Sachs
196. A patient comes to the clinic complaining of muscle weakness. CBC analysis shows hypomagnesemia and hypokalemia. You diagnose your patient with Familial Hypokalemia-Hypomagnesemia. Where in the nephron would the channels be affected if this disorder manifested from a deficiency in the SLC12A3 gene?
-
Glomerulus
-
PCT
-
Thick Ascending Loop
-
DCT
-
Efferent Arteriole
197. A patient comes in with a distended abdomen that is tender to palpation. You take an ultrasound of his abdomen and notice countless cysts on both of his kidneys. Gene mapping shows a deficiency of the PDK1 gene. Which disorder are they suffering from?
-
Adult Polycystic Kidney Disease Type 1
-
Adult Polycystic Kidney Disease Type 2
-
Infantile Polycystic Kidney Disease
-
Alport Syndrome
-
Von-Hippel Lindau Syndrome
198. A 10 year old child was brought to the ER because he suffered from stomach cramps during kickball that got so bad he collapsed and scraped his kid knee. His mother tells you that he was born with infantile polycystic kidney disease. Which gene is deficient in this child?
-
COL4A3
-
PDK1
-
PDK2
-
VHL
-
PKHD1
199. You are shown a brain MRI of a patient that suffers from a deficiency of the VHL gene and notice several hemangioblastomas. Which disorder matches the disorder this patient suffers from?
-
Huntington’s Disease
-
Fragile X Syndrome
-
Becker Muscular Dystrophy
-
Xeroderma Pigmentosum
-
Cystic Fibrosis
Session 108 – Endocrine System Histology I
200. The anterior pituitary is derived from which of the following?
-
Glandular endoderm
-
Intermediate mesoderm
-
Neuroectoderm
-
Oral ectoderm
-
Splanchnic mesoderm
201. Parathyroid hormone is secreted primarily by which cell type?
-
Acidophils
-
Basophils
-
Follicular cells
-
Oxyphil cells
-
Principal cells
202. A patient presents with Addison’s disease, showing low levels of testosterone. Which of the following layers of the adrenal gland is most likely affected?
-
Capsular cortex
-
Zona fasciculata
-
Zona glomerulosa
-
Zona granulosa
-
Zona reticularis
203. Which of the following secretory cells is an acidophil?
-
Adrenal corticotropin-releasing cells
-
Gonadotrophs
-
Lipotropin-releasing cells
-
Mammotrophs
-
Thyrotrophs
204. On a histological slide how can the pars intermedius be distinguished?
-
Absence of basophil infiltration
-
Absence of corticotrophs
-
Presence of chromophils
-
Presence of cysts (large, white-stained circles in H&E staining)
-
Presence of nervous tissue
Session 109 – Endocrine System Histology II

205. In the picture above, 1 is referring to which tissue?
-
Thyroid
-
Parathyroid
-
Anterior Pituitary
-
Posterior Pituitary
-
Adrenal Medulla

206. Number 1 in the picture above refers to which type of cells?
-
Follicular cells
-
C cells
-
Chief cells
-
Oxyphil cells
-
Glomerular cells
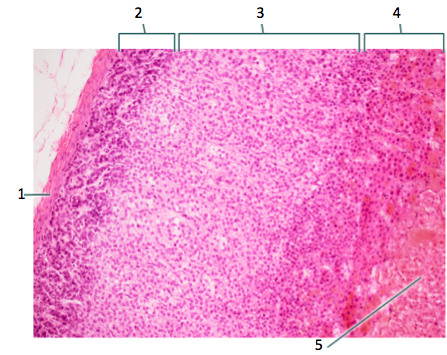
207. In the picture shown above section 5 secretes which of the following?
-
Aldosterone
-
Androgens
-
Catecholamines
-
Mineralocorticoids
-
GLucocorticoids

208. Which of the sections in the image above functions similarly to a sympathetic postganglionic neuron?
-
1
-
2
-
3
-
4
-
5
209. Which of the sections in the image above would likely NOT be affected in an individual with Addison’s disease?
-
1
-
2
-
3
-
4
-
5
210. Which of the sections in the image above secretes a glucocorticoid?
-
1
-
2
-
3
-
4
-
5
211. Which of the sections in the image above functions primarily on the distal convoluted tubule of the nephron?
-
1
-
2
-
3
-
4
-
5

212. Identify the tissue shown in the histology image above?
-
Thyroid
-
Parathyroid
-
Pineal Gland
-
Anterior pituitary
-
Posterior pituitary
213. What is the major function of the tissue in the image above?
-
Increase calcium levels
-
Decrease calcium levels
-
Circadian rhythm regulation
-
Sodium reabsorption
-
Generation of secondary sex characteristics